
By Raul Palacio Rodriguez BDS MHA
Dental decay or caries is the most prevalent chronic disease in the world. Almost 100% of adults have experienced this pathology mostly in developing countries (Petersen et al., 2005). As a basic definition, caries is the destruction of susceptible dental hard tissues by the action of acids which are produced as metabolites of bacterial fermentation of carbohydrates (Selwitz et al., 2007). It is a transmissible chronic oral disease that can start at early ages and continuing its development during the whole lifetime of an individual (Selwitz et al., 2007).
Caries entails both clinical and non-clinical consequences. Clinically speaking, this pathology not only affects dental hard tissues; caries also allows the entry of microorganisms to maxillofacial zones that may result in pain (sometimes extreme), reductions in the functionality of craniofacial structures and occasionally death. Non-clinical consequences are related to the infrastructure and workforce needed in order to treat the huge burden of this disease, the productivity losses of patient on her/his family or the nonattendance to educational institutions. Due to its prevalence and characteristics caries is the most expensive oral pathology to treat.
Irrespective of the level of development in society, the distribution of caries among the population is heterogeneous. Nevertheless, evidence suggests that people from lower socioeconomic status background are more prone to experience caries (Selwitz et al., 2007). Measuring inequality in oral health is, however, not straightforward since they depend on age groups, generational cohort and the dental index used to measure (Steele et al., 2015). A core reason is given by the multiple factors that are linked to caries and its presentation as a chronic disease. Harris et al. (2004), for example, systematically reviewed 73 studies, showing that 106 risk indicators were significantly associated with the prevalence of caries in young children.
How to treat caries
Undoubtedly the best way to treat caries is avoiding the occurrence of them. Unfortunately, most national health services are oriented to solve problems from the traditional perspective on the basis of filling or extracting teeth once caries has already happened. This phenomenon may be explained partly due to the high cost of oral health services, the multifactorial character of this disease or the fact that this pathology can act throughout the lifetime.
Fluoride
The use of fluoride is the most significant intervention to prevent the occurrence of caries and, among all methods of fluoride delivery, fluoridated water is the most important. Despite fluoridated water has been in use for almost 70 years (Mullen, 2005) and the evidence confirms this method is safe, population’s acceptance of it is low (Rabb-Waytowich, 2009); indeed, only 10% of population in UK has a optimally fluoridated water ( 1.0 mg/l) (BFS, 2013) – See Figure 1.
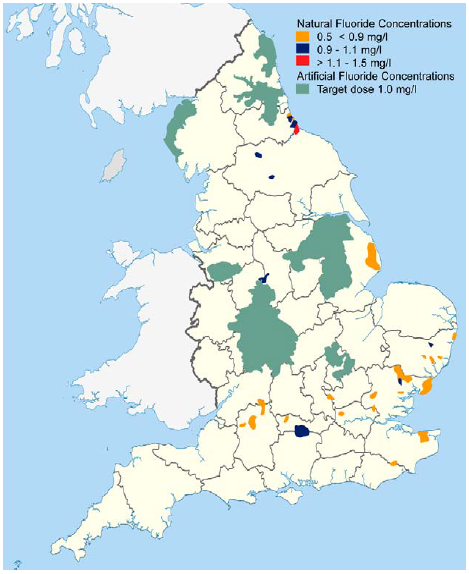
Fig 1. Fluoride concentration in water supplies from British Fluoridation Society webpage.
So, what must be done when the societies reject the use of fluoridated water?
Other options
The health care market is constantly developing new technologies. Dentists in developed countries are equipped with a variety of products which can be applied in the clinical setting to prevent the occurrence of caries. Examples of these may be equipment to count of S. mutans, sealants, glass ionomer cement, fluoridated gels or fluoridated varnishes. Likewise, they can prescribe different kinds of mouthwash, toothbrushes and toothpastes as well as control their patients with an additional check-up. However, what does happen in countries without the budget for an oral health care system based on clinical setting appointment?
These questions lead to the development of innovations by the health institutions. Innovation does not mean just replicating a programme that was successfully in other places, since a good experience in a clinical setting (or place) does not necessarily imply similar outcomes in others. Factors not always related to clinical setting such as logistics or the institutional framework may explain this discrepancy.
Good decision-making in oral health
In order to ensure they are making a good decision and that an oral health strategy is well implemented, decision-makers must consider the most relevant factors that produce caries and the context where the programme is applied. So, decision-makers have to decide wisely about how spend their budgets.
A randomized control trial (RCT) could help to make a decision. However, RCTs that include all comparators (technologies either for prevention or treatment) are expensive and not easy to do. Also, due to their controlled nature they have not able to reflect properly the “real world”. So, a RCT would not be the best alternative for a decision-maker that wants to take into account his/her budget constraint in a more realistic scenario; a better option is to use some tools provided by health economics such as economic evaluation (EE).
There are a large number of EEs done in medicine which have strongly influenced clinicians, policy makers, health services managers and patients. However, despite the increase during the last 10 years, there are comparatively few EEs in dentistry than medicine and, the number of high-quality evaluations is even fewer (Culyer and Newhouse, 2008, Marino et al., 2013).
Conclusion
In conclusion, caries is a preventable chronic disease, associated with several risk indicators and is very expensive to treat. In order to reduce clinical and non-clinical consequences, health institutions have to analyse new technologies in dentistry not just from the clinical perspective, they have to consider more scenarios. Economic evaluations and hence, health economics, can be an alternative to decision-makers, giving them information to make a more accurate decision about dental programmes.