The kynurenine pathway is responsible for the catabolism of the essential amino acid kynurenine. This pathway has been linked to acute and chronic pain in animal models of viral infections. Research by the team has shown upregulation of this pathway in pulpititis (toothache) and it appears to be pushing the pathway towards neuroinflammation and pain. This project therefore looks to examine the kynurneine pathway as a means to therapeutic reduce the pain experienced during toothache and potentially persistent pain which can follow. 2. There is an absence of topically applied medications for use in managing dental pain. Much of this is due to the complexities in examining potential therapeutics with animal models often used. This project looks to develop a lab made (in vitro) cell model of dental pulp using stem cells. This will reduce our reliance on animal models in keeping with the NC3Rs, but also speed up drug screening as compounds can be assessed more easily and at a greater range of doses prior to further investigation ensuring only the most promising are taken forward.
The way that people understand pain is important. Typically, believing that pain is caused only by physical factors and using only passive modalities of treatment are both associated with a poorer prognosis. Unfortunately, this is exactly what many people do believe about pain including some health professionals! A recent project carried out by students from the school of Psychology explored whether adding experiential methods could improve traditional methods of pain education.
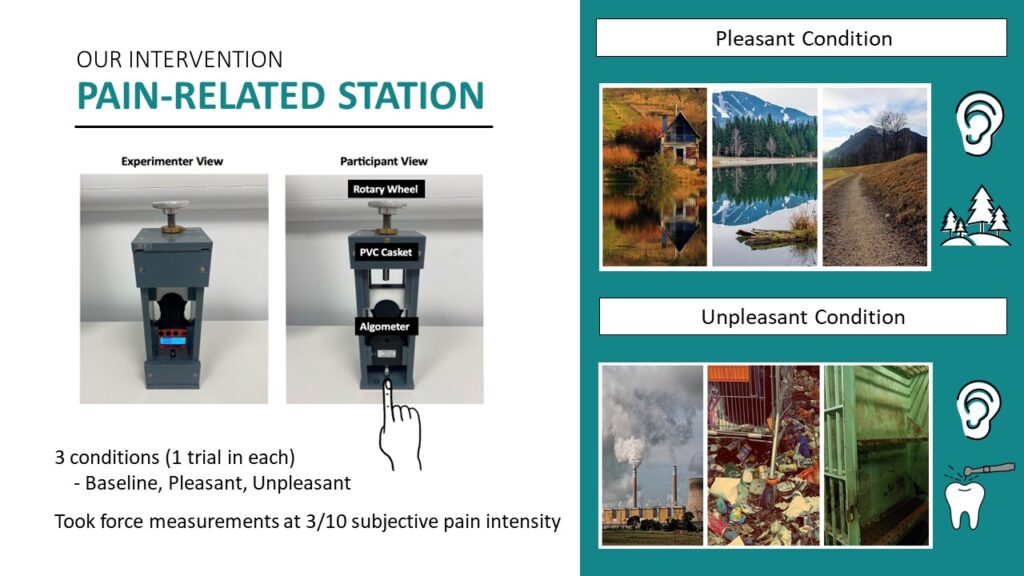
The study recruited 60 participants from the student and local communities. Each participant engaged in 3 learning activities about pain in a randomised order – watching an information video on YouTube, engaging in a pain-related experiential task and engaging in a sensory experiential task.
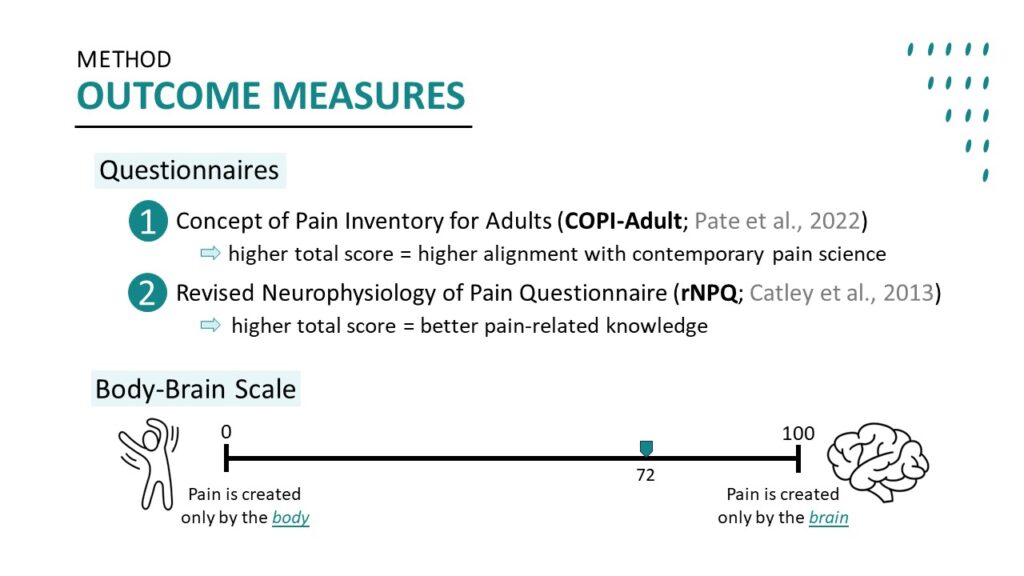
The pain-related sensory task used a finger press that applied pressure to participants’ middle finger until they declared their pain to be at a level of 3 out of 10. All participants completed this task first in a neutral condition and then in randomised pleasant or unpleasant conditions. The difference in pressure applied to reach the agreed threshold in each condition was immediately fed back to each individual. Beliefs about pain before and after each task were measured by a “body-brain scale” on which participants were asked to indicate their beliefs about whether the body, or brain was more important to the experience of pain, in addition to overall measures for change in belief.
The research showed that, although watching a video led to the largest change, participation in the pain experience station further increased the participants’ beliefs about the role of the brain in pain. Experiential methods appear to have promise in changing unhelpful beliefs about pain.
MiTiGate Trial: Managing chronic Myalgia Temporomandibular Disorder: a pragmatic randomised controlled trial of Botulinum toxin type A, lidocaine, and amitriptyline/gabapentin, with internal pilot and cost-effectiveness analysis
Temporomandibular disorders (TMD) affect the jaw joint and its muscles in 1 in 15 people. The most common TMD is “myalgia” TMD or “masticatory myofascial pain” (M-TMD). M-TMD causes pain in the jaw muscles and interferes with daily activities, for example, chewing, eating and talking, and worsens quality of life.
Self-management advice provided by dentists and doctors is helpful for M-TMD. However, up to 49% of people still suffer life-long pain, known as chronic M-TMD. People who develop life-long pain are referred to a hospital for specialist treatment.
Hospital specialists often use tablet treatments such as amitriptyline or gabapentin as the next step to reduce pain. However, newer treatments are available. These newer treatments involve injections of a “muscle relaxant” (Botox) or a “numbing” agent (Lidocaine) directly into the painful muscles.
Unfortunately, no high-quality evidence is available to help guide the specialists’ decisions on which of these treatments is the best next step.
Therefore, we will aim to generate the evidence needed by conducting a UK-wide clinical trial. We will recruit 663 people with chronic M-TMD from hospitals, medical and dental practices, and through different types of adverts and community engagement. We will randomise (allocate by chance) people into one of three groups: 1) usual treatment (amitriptyline and/or gabapentin medications); 2) Botox injections; or 3) Lidocaine injections. Each person will have an equal chance of receiving each treatment and will be told which treatment they are receiving. Medications will be monitored and adjusted, and the clinical team will provide injections every three months for those receiving them. Each treatment will continue for nine months.
Before recruiting large numbers of people, we will run a mini version of the trial called a “pilot study” to make sure what we are planning works well. We have already acted on lots of feedback from patients, doctors, and dentists to try to avoid any problems.
Patients have told us the best treatment must improve quality of life and reduce pain; the cost of treatment to the NHS is also important. Therefore, we will measure patients’ quality of life and pain intensity after treatment. We will also examine treatments’ value for money. To understand people’s experiences of the trial and each treatment, we will invite up to 30 participants to interview to share their views.
Minimising side effects is also crucial for patients; they worry Botox may affect the bone of the jaw joint. We will explore this in a small group of patients in the trial, using scans of the jaw joints; these don’t require radiation.
We will keep patients and the public involved during the trial through our patient and public involvement/engagement co-applicant and advisory group. Our previous creative patient and public involvement/engagement work, e.g. stand-up comedy and animations, will help us to capture people’s attention and explain things in an easy-to-understand manner.
We are currently looking for people in the northeast of England with ME/CFS, Temporomandibular Disorders (TMD), or neither of these conditions to take part in this study. If you are interested in taking part, please email james.allison@newcastle.ac.uk for more information.
Summary of the study
Widespread pain affecting the muscles and joints is a significant problem for people with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), and has a huge impact on their everyday activities and quality of life. While central sensitisation in the brain and dysfunction of the autonomic nervous system (ANS) are thought to play a role, the precise mechanisms involved are not yet known.
Temporomandibular disorders (TMD) are a group of musculoskeletal conditions affecting the muscles that move the jaw. They cause pain in the face and jaw, and are more common in ME/CFS than in the general population. Preliminary work suggests that the link between ME/CFS and TMDs may be due to a common underlying problem affecting the ANS.
The ANS controls many of the unconscious activities of the body such as breathing, heart rate and the circulation of blood. It is known to work less well in ME/CFS, and is worse still when TMD is also present.
James Allison, investigator on the Elucidate study sets up EEG equipment in the lab.
The aim of this study is to explore how brain activity in response to pain is different in these conditions and whether the ANS plays a part. We will use electroencephalography (EEG), which measures the electrical activity of the brain, to assess the brain’s response to painful pressure applied to the finger and jaw in people:
with ME/CFS only
with both ME/CFS and TMD
with TMD only
without ME/CFS or TMD
We will also use non-invasive stimulation of the vagus nerve to modulate the ANS, and to measure the effect this has on brain activity in response to pain.
We hope that this study will help inform future treatments for pain in ME/CFS and TMD by identifying where in the brain any differences occur, and what part the ANS plays.