In my last blog post I discussed the use of a gene-editing technology, termed CRISPR, and the controversy surrounding its potential for use in human studies. Today I will talk about an experimental gene therapy, distinct from CRISPR, that has been used to restore the immune systems of young children with X-linked severe combined immunodeficiency (SCID-X1).
SCID-X1 is caused by mutations in the gene that encodes interleukin 2 receptor common gamma chain (IL2RG), located on the X chromosome. As a result, these children are unable to produce two essential types of immune cell, T cells and natural-killer (NK) cells. Furthermore, functional T cells are required for the proper development of B cells and so these patients also possess a defective B cell population. For those that suffer from this disease the lack of a functional immune system means that infection with viruses or bacteria, that a healthy individual will often fight off, can actually be fatal. As a result, unless they are cured, these children are destined to a life of isolation.
The current gold standard in therapy entails undergoing a bone-marrow transplant from a matched donor. However, this is not always possible and so scientists around the world have sought an alternative therapy, for almost two decades. One potential treatment involves delivering a functional copy of the IL2RG gene into the children’s cells using a viral transporter, consequently restoring their immune system. Historically, trials utilising this method have had mixed results, leading to only partial restoration of immune function. Moreover, early trials led to some children developing leukaemia through unintentional activation of proto-oncogenes, highlighting the risks associated with the technology.
On the 17th April scientists published the results of a study wherein 8 infants with SCID-X1 were treated using the same approach; however, researchers utilised a different virus. This version is better at delivering IL2RG to slowly-dividing stem cells, which will eventually form the patients’ immune cells. Encouragingly, all of the children who underwent this treatment went on to produce the essential cell types required for a functional immune system, T cells, B cells, and NK cells. Furthermore, up to 2 years after treatment the children are showing no signs of leukaemia. The results of this study mean that these children, that would otherwise be unable to leave the protective confines of specialist hospital facilities, are now living normal and healthy lives.
This study represents a landmark improvement in the treatment of patients with SCID-X1. However, it is too early to tell whether this treatment is a permanent cure for the disease. It is not known how these children’s immune systems will function in the long-term. Is it possible that the effects will wear off? For now, the restoration of immune function alongside improved quality-of-life is an indisputable success for these patients.
An ever-expanding number of frontiers of novel and revolutionary treatments is being explored by scientists in their efforts to combat Parkinson’s disease (PD).
A new trial, outcomes of which were published this month in Brain, tested the clinical efficacy of delivering a neurotrophic factor called GDNF directly into the brain area affected by the disease. When glial cell-derived neurotrophic factor (GDNF) was first identified along with the other factors, it was trialled in animal models of the disease and showed promising results. For instance, in rodent models of PD, which use a toxin that specifically targets dopaminergic cells that are lost in the course of disease, supplying GDNF factor was found to preserve those neurons previously exposed to the toxin. Neurotrophic factors essentially act to block any programmed cell death of neutrons and increase the number of signalling molecules that allow the cell to survive and proliferate. Their sole function seemed to be the much-anticipated key to reversing neuronal cell death and loss in PD.
Unfortunately, the subsequent randomised, double-blinded trial assessing the efficacy of administering GDNF directly into putamen did not find any statistically significant differences between treatment and placebo groups. Both groups showed a decrease in motor symptoms, potentially owing to the effect of placebo in such clinical trials, hindering clear understanding of the effects of the agent in question. However, almost half of all patients who had GDNF administered (compared to none from the placebo group) had a large decrease in their motor symptom score. Moreover, it was found through positron-emission tomography (PET) scanning that dopamine precursor uptake was significantly greater in the GDNF-treated patient group, indicating that dopaminergic cells in those patients are synthesising dopamine in higher amounts and hence are more actively functioning compared to the placebo-treated group. This indicates that this treatment and treatment with other neurotrophic factors, if administered using the same revolutionary delivery method, still hold promise if tested again in a wider setting of patients. The failure of this trial in part, in my opinion, could be explained by the relatively long duration of the disease (over 5 years since motor symptom onset). If this disease duration is decreased in subsequent trials, better results might be expected, as a greater number of neurons is lost the longer it has been since diagnosis. Therefore, if the factor is given at the earlier stages of the disorder, it may prevent the irreversible loss of vulnerable neurons that drive the progression of the disease.
Earlier this week, I attended a very successful seminar in the School of Pharmacy Newcastle University. Entitled ‘Optimising medications for people with limited life expectancy’, this seminar could only be a great opportunity to find out about factors affecting our prescribing culture, not only in the UK, but in western world in general.
Basically, the main point of the speaker Dr Adam Todd, Reader in Pharmaceutical Public Health, School of Pharmacy was to showcase the current evidence on surplus medication prescribed for elderly people with late stage diseases with limited life expectancy according to predictions of clinicians. De Todd had extensive experience in lung cancer patients who have been prescribed medication ‘for life’, which at some point lose their purpose and should be discontinued. However, no clinician or pharmacist would easily review the medication list of those patients unless an adverse drug reaction or change in their clinical response appeared. In many cases, patients are under the impression that they really shouldn’t discontinue any medication, without understanding of the actual effect of the particular drug to their bodies. Therefore, even if the need to discontinue a specific therapy is pointed out to them, their lack of education doesn’t allow them to accept the proposal as a positive change, but rather return to a different prescriber with the desire to leave with a prescription for the exact same drug.
Guidelines fail to consider situations like this and they don’t provide recommendations on discontinuation of a medication if its mostly preventative nature is no longer useful for the patients and could only continue reducing their quality of life. Healthcare professionals are not aware of the consequences of unnecessary medication for the patient either. Therefore, the vicious circle continues and leaves those who understand the problem with the only option to raise awareness in scientific conferences and informal chats.
With all current information and guidance available about prescribing, is it time to look the other way and reduce the load of polypharmacy that heavily strikes the elderly population and costs millions to the NHS each year? The change is in front of us; we just have to learn and go with it.
Deoxyribonucleic acid (DNA) is the backbone of the natural world and the molecule which encompasses all of the information needed for the survival of most living organisms. It exists at its most primary level as a series of nitrogenous bases within nucleotides, of which there are 4: Adenine (A), Thymine (T), Cytosine (C) and Guanine (G). These 4 bases form hydrogen bonds with one another in particular patterns; A pairing with T, and C pairing with G, to form the double helix structure that is associated with the DNA molecule as a whole. It’s rather incredible that the information needed to grow and maintain a living organism comes down to 4 nitrogen bases.
Imagine what could be done with 8 letters; 8 bases.
This is what a group of researchers from various US companies and institutions have managed to create: eight-letter DNA, known as Hachimoji DNA. By tweaking and tailoring the structures of the regular bases, they made synthetic molecules that have the correct properties to be incorporated into the natural DNA structure. This DNA molecule would have the potential to store twice as much information as regular DNA and is thought to have possible applications within technology and data storage in the future.
Building on the existing DNA framework
Considering that the process of gene expression from DNA is the product of millions of years of evolutionary fine-tuning, it is unsurprising that scientists wanted to take the DNA model further and try to apply its template in new ways. It is, after all the most efficient way of storing and expressing vast quantities of information known to man.
The Hachimoji DNA is comprised of the four natural bases, as well as four more synthetically-made nucleotide bases, P, B, Z and S. These are each similar in shape to one of the natural bases, with slight variations in their bonding patterns. Within the four synthetic bases, S pairs with B and P pairs with Z. The research group created hundreds of Hachimoji double helixes with different combinations of the natural and synthetic base pairs to test whether they had to correct properties required to support life in the same way as ordinary DNA.
The characteristic property of DNA is its durability – no other genetic molecule is as stable or predictable. As a result of this, the four nitrogenous bases were always thought to be unique, but it turns out that the new synthetic DNA bases in Hachimoji DNA seem to behave in a similar way. The study has found that even after creating hundreds of Hachimoji molecules, the synthetic bases always bound to their complementary counterpart predictably. The researchers also managed to show that the double helices of the synthetic DNA remained stable no matter what order the bases were in. This is a crucial property of DNA which has allowed evolution and the survival of living organisms, as for this to happen helices must remain intact even if there is variation in the base sequence.
The final hurdle in this investigation was to prove that the synthetic, 8-letter DNA could not only store information, but that it could be read, transcribed and translated by enzymes into RNA. With this in mind, the researchers developed synthetic enzymes which actually successfully copied Hachimoji DNA into Hachimoji RNA! All of their results so far suggest that this synthetic hybrid molecule has the potential to act like the “real deal”.
It’s an exciting development in our understanding of evolution and the universe as a whole. It has been described as a conceptual breakthrough that natural DNA bases are not the only molecules that can form this stable and so-far unrivalled genetic material (DNA). According to Steven Benner, senior author of the research paper for this study, this strongly suggests that alternative structures like Hachimoji DNA could exist elsewhere in the universe, allowing for the evolution of life elsewhere – although it might look very different to life on Earth!
Most scientists will have heard of genome editing in some form or another; whether it’s altering the genes of a cell line through radiation or targeting specific regions of the genome by inserting additional base pairs or entire genes. Undoubtedly, a large proportion of the general public will also have an idea as to what genome editing means, even if it is as a result of watching Jurassic Park! Due to recent advances in DNA editing technology, the prospect of using the technique to alter the genome of a human being is now less fantasy than reality. But even if we could edit our own DNA, does that mean we should?
Last year, scientists were forced to answer this question when the first genome edited babies were born, despite the practice being against government regulations. He Jiankui, a geneticist from the Southern University of Science and Technology of China, took to YouTube in November 2018 to announce his controversial studies. Jiankui claims that he successfully edited the DNA of human embryos using a technology called CRISPR-Cas9. These embryos were then implanted by IVF and 9 months later the first genome edited babies were born. But what part of their DNA had been edited and why? Jiankui claims that, using CRISPR-Cas9 technology, he was able to disable a gene called CCR5. This gene encodes the CCR5 receptor which allows the HIV virus to enter cells and by disabling it, theoretically, the virus cannot infect them. On the surface this might sound like a great idea; if we can prevent a disease then surely it must be beneficial?
However, the general response from the scientific community has been one of public outcry. Many view Jiankui’s use of the technology as being both dangerous and irresponsible. Scientists are yet to reach a consensus as to how genome editing technologies such as CRISPR-Cas9 should be used. Despite the potential benefits there are a great number of risks associated with such techniques, both scientifically and morally. Although genome editing may be used to prevent disease, it has the potential to be used for ethically questionable purposes, such as to select for specific traits. Further to this, it cannot be guaranteed that by editing one part of the genome you do not affect another, which could have disastrous consequences. In Jiankui’s case, experts have stated that there was no reason to have edited these babies’ DNA, as although the father was HIV-positive, there is no real risk of transmission. Furthermore, HIV-positive mothers are able to undergo caesarean section to avoid transmission of the virus. The Southern University of Science and Technology of China has stated that they were unaware of Jiankui’s research. The university have launched an independent investigation into his claims.
Genome editing has been and remains a controversial topic, and it is likely He Jiankui’s studies will have only reinforced the cautioned stance that the scientific community holds.
As the reality of climate change becomes more and more apparent and governments seem to be slow in implementing the changes needed to prevent temperatures rising above accepted limits, I’ve been thinking more about my diet. Cutting down on meat and dairy should be a no-brainer, given that their production uses 83% of farmable land and makes up for 60% of carbon emissions in the food industry. It also becomes a valuable tool for engagement when feeling powerless in the face of melting glaciers and slow-moving politics. While lentils and beans are a common way to replace meat in many recipes, there’s one option I haven’t explored yet: Insects.
While eating these chitin-covered delicacies is far from uncommon – it is estimated that over 80% of nations eat insects – I personally haven’t had far more experiences than the crispy honey-glazed grasshopper that came as part of a novelty gift. But would eating more insects solve some of the problems that come from rearing much larger livestock?
A lot of reasons speak for eating insects: studies have found that to rear the same amount of insects, over 10 times less biomaterial is needed compared to meat. Furthermore, they have extremely fast life cycles, increasing in body weight and size much faster than mammalian livestock. They are also nutritious, providing not only a source of protein and unsaturated fats but also amino acids, of which people who have mainly grain-based diets are often deficient.
However, there are also some caveats. While insect farming was generally found to be positive, dwindling wild insect populations could be further diminished by people ‘foraging’ them from their natural habitats. Another problem is the negative attitude especially western culture has towards eating insects, which could prove difficult when introducing these ingredients into the market.
I’m definitely open to including insects into my diet, even if to demonstrate that there is a market and a demand for more sustainable products. However, I will see how the next evening with friends goes when I proudly serve them some vegetable soup with a garnish of salty mealworms…
——–
If you would like to know more about eating insects, check out these resources:
Mediterranean diet, characterised by consumption of fish, olive oil, greens and grains, has been associated with healthier lifestyles and prolonged lifespan. Japanese diet has also been associated with longer lifespan, and the intake of fish and fish oils is prevalent in the Asian diet. Western diets, however, are largely based on meat products and a widespread use of butter, both of which are rich in saturated fats and cholesterol, which have been established to contribute to atherosclerosis. Atherosclerosis is a term for a pathological process that leads to a build-up of fat and inflammatory cells, eventually forming an atherosclerotic plaque within the walls of coronary arteries that supply the heart itself with oxygenated blood. If untreated, atherosclerotic plaques may cause heart attacks if the arteries’ lumen becomes too narrow to adequately supply the cardiomyocytes with oxygen and glucose.
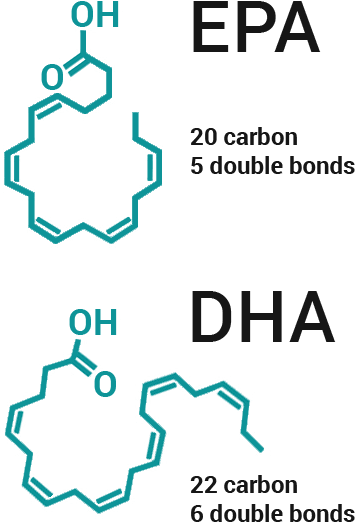
What is the difference in oils and fats and how do we know which one is more likely to be beneficial? There is some evidence suggesting that increased intake of saturated fatty acids that only have single C-C bonds between the carbon atoms in their skeleton is not beneficial and might be damaging to cardiovascular health, whereas unsaturated fatty acids are considered “healthier” for the heart. Unsaturated means there is at least one or more double C=C bonds present within the fatty acid structure, called mono- and polyunsaturated fatty acids, respectively. But in biology nothing is ever quite so simple. A lot of fish oil supplements trials concluded that fish oil had no effect on protecting against cardiovascular diseases and scientists were trying to untangle whether some fatty acids and not the others could be beneficial.
An observational study conducted in Denmark and published this January in journal Stroke has ruled out that higher amounts of EPA are more beneficial than for example DHA in reduction of stroke associated with lower blood supply to the brain, called ischaemic stroke. Both of those fatty acids belong to the class of polyunsaturated fatty acids and are more commonly known by the name of omega-3s.
A clinical trial, REDUCE-IT, has compared EPA with placebo to identify if EPA may indeed reduce the rates of stroke in subjects. Indeed, they have found that the rate of strokes in the group of subjects that were taking high levels of purified EPA were decreased by almost a third compared to the control group taking placebo.
Therefore, it is important to address over-the-counter fish oil supplements and the proportions of different fatty acids that are within those oils and whether the level they are present at would cause an effect on reducing the risk of myocardial infarction and stroke. The balance and proportion of EPA to DHA may also determine this.
There are many other extremely important factors that determine the risk of cardiovascular diseases and must not be forgotten, including genetic predisposition, alcohol intake, smoking, unhealthy sleep patterns, age, lack of physical exercise, as well as diet. In the era of global obesity ‘pandemic’ we need to pay closer attention to our diet and make sure it is varied and balanced.
Publishing research results in scientific journals is crucial for research dissemination within the scientific community. The impact and quality of a research project can be demonstrated by the journal it is published in. For all research projects, as long as they are scientifically sound, legitimate and well designed, there is a journal that is appropriate. However, sometimes we aim high and without taking into account the competition in the field and the scope of the target journal, which can be very disappointing at times. In order to avoid a potential rejection, there are certain steps to be followed.
1. Identify a few target journals in advance
The main factors to consider when choosing journals is not only the impact factor, but also the scope of the journals of interest. For example, a specific haematology journal might not accept a manuscript about the pharmacology of an anticoagulant drug in vitro. It is always good to aim higher, but it might take more time to identify a journal that meets your criteria. On the other hand, if the manuscript gets rejected you’d have to repeat the steps all over again. However, the worst case scenario is your manuscript is rejected before getting to reviewers, in which case, you would have no clue what to improve before re-submitting to another journal. If you do get through to reviewers, and the rejection comes as a result of their comments, then this is your opportunity to use the feedback and improve your manuscript to hit another top journal.
2. Format your manuscript according to author guidance of the journal
Paying close attention to the journal’s guidelines for submission shows the dedication, the attention to detail and the professionalism all good quality journals will look for in their authors. If you can’t be bothered to read their 10-page guidance and even identify the category your manuscript falls in, then don’t expect to get a positive response back.
3. Write a good cover letter
Your letter to the editor should be polite, professional and succinct. Dedicate enough time to make sure that, firstly, there are no typos and, secondly, it contains a good answer as to why your manuscript is relevant to the journal and what is the overall impact of your research. The stronger the impact you (and your results) can demonstrate, the more time the editor will spend on your abstract, hence you’re more likely to reach the review stage.
4. Submit according to the guidance (pay submission fees)
Some high impact journals may ask for a fee, but don’t be put off by that. Follow the steps, spend some time to review the final version of your manuscript, to upload all necessary documentation and tick all those boxes appropriately. Again, the editor will use the information submitted to inform the selection of reviewers, if they are happy with the first impression of your work.
Even if you do get a rejection, which happens in nine out of ten cases, there is nothing wrong with resubmitting to a new journal. The process will start over again, but you’ll certainly find things to improve. After all, your confidence and belief in your own research output is a necessary ingredient of your academic life.
As this year comes to a close, it feels right to reflect on the accomplishments that have been made by researchers at Newcastle University (with collaboration from other institutes) this year. The academic output of the University as a whole is, of course, extremely widespread, so I will be focusing on a small fraction of the research progress made in the Medical Sciences this year.
1. Fighting against drug-resistant Tuberculosis Tuberculosis is usually treated by the antibiotic rifampicin; however, in recent years strains of Mycobacterium tuberculosis (TB-causing bacteria) have become resistant to it, making treatment very difficult and raising concerns over potential epidemics. Tuberculosis can be fatal without treatment and drug-resistant strains may become more prominent, leading to increased deaths worldwide. Newcastle University and Demuris Ltd researchers have made a promising discovery in a naturally occurring antibiotic called kanglemycin A. This antibiotic works in a similar way to rifampicin but has been identified to be active in working against Mycobacterium tuberculosis that are resistant to rifampicin. This is due to kanglemycin A’s ability to bind with stronger affinity to the RNA polymerase molecules of the resistant strain. This discovery can be used in drug development in the future in order to prevent any further fatalities from rifampicin-resistant tuberculosis.
2. The first 3D-printed human cornea The cornea is a fundamental part of the eye which acts as the outer-most lens, while preventing microbes, dirt and dust from entering. The cornea can become damaged due to injury, infection or conditions that cause corneal swelling, such as Fuchs’ endothelial dystrophy. There is often a shortage of corneas available for transplantation in people who need them, meaning that patients suffer visual impairment and potential blindness. These scientists at Newcastle University have devised a technique that uses stem cells from the corneas of healthy donors to create a “bio-ink”. This ink is then used in a 3D bio-printer to form the shape of a human cornea in under 6 minutes! The stem cells then use this as a template to grow into a cornea that can be used for transplantation. Although this method is a while away from being available to the general public it is an extremely exciting and influential development!
3. A new link between Tuberculosis and Parkinson’s disease This collaborative study led by Newcastle University, the Francis Crick Institute and GSK suggests that drugs we design for Parkinson’s disease might actually be able to treat tuberculosis as well. At the moment the focus for Parkinson’s treatment is to make drugs that block LRRK2, a protein which becomes overactive in the disease due to mutations in the LRRK2 gene. The results from this study indicate that this LRRK2 protein prevents the clearance of Mycobacterium tuberculosis by stopping phagosomes fusing with lysosomes in the immune response. Therefore, a drug that blocks LRRK2 protein could potentially be useful in helping the immune system to fight a tuberculosis infection.
4. Further insights into reversing Type 2 diabetes This study, funded by Diabetes UK, set out to decipher why some patients with Type 2 diabetes can recover to regular health through weight loss, and why other patients cannot. The study used data from a subset of individuals already taking part in the DiRECT (Diabetes Remission Clinical Trial) study which used non-surgical weight management to see whether it would lead remission of the disease. The researchers at Newcastle saw that there was one main difference between those who responded to the weight loss (and entered remission) and those who did not. The ‘responders’ had insulin-producing beta cells that appeared to start secreting the correct amount of insulin again after losing weight, while ‘non-responders’ had no change in insulin production despite weight loss. Responders were generally found to have lived with Type 2 diabetes for slightly less time on average than non-responders, which suggests that if beta cells are not under stress from increased fatty deposits for too long, they may still be able to recover when fat loss occurs.
5. Improvements in treatment for bone marrow cancer Myeloma is a type of blood cancer that develops from plasma cells within the bone marrow. It has a 5-year survival rate of 50% and there is no complete cure, but there are ways to treat and manage the cancer in order to increase the amount of time patients survive for. In a study published by The Lancet Oncology, researchers at Newcastle and Leeds University monitored over 4000 patients in the UK for 7 years, in order to assess the efficacy of the drug lenalidomide (not yet available on the NHS). The patients had already completed their initial treatment and some were then randomly chosen to use lenalidomide during drug therapy. The results showed that lenalidomide significantly extended the lives of the patients and it reduced the risk of cancer progression or death by more than 50%. This study therefore shows a very promising new treatment method for people living with myeloma, which hopefully will be seen within the NHS before too long.
These publications are representative of just a tiny amount of the work at Newcastle University that has had global success this year, and some additional links are listed below. Look out for more North East research developments in 2019 – happy New Year!
——–
If you would like to learn more about life science research news from Newcastle University please follow the links: https://www.ncl.ac.uk/medicalsciences/news/ & https://www.ncl.ac.uk/press/archive/
Breakthrough in childhood brain cancer
Tobias Goschzik PhD, Edward C Schwalbe PhD, Debbie Hicks PhD, Amanda Smith MSc, Anja zur Muehlen, Prof Dominique Figarella-Branger MD et al.
Potential to use gene-editing to halt kidney disease
Simon A. Ramsbottom, Elisa Molinari, Shalabh Srivastava, Flora Silberman, Charline Henry, Sumaya Alkanderi, Laura A. Devlin, Kathryn White, David H. Steel, Sophie Saunier, Colin G. Miles, and John A. Sayer