Northern Pride brought record numbers to Newcastle this year, partnering with NE1 to provide “a more accessible, unapologetically visible pride celebration”. In a pivot from the regular venue of the Town Moor, the Pride in the City festival sprawled entertainment across the city centre in a three-day takeover. As well as stalls and music filling the streets around Greys Monument, the event also saw families enjoying free crafts in the Assembly Rooms, local LGBTQ+ artists performing at the Curious Arts Stage, and party-goers heading to the ticketed arena in Times Square.
Sitting down for lunch on the Grey Street astroturf, we adjusted to the new surroundings. Among the bustle of shoppers and stallholders, the more open atmosphere of the Town Moor was certainly missed. But it was preferable to last year’s arrangement, where the financial pressures on the event were depressingly evident; half of the field had been barriered off as a VIP zone, and those of us unwilling to pay the ticket price peered over the metal fence in annoyance to get a view of the entertainment we’d previously taken for granted.
The new programme seems to have been a hit for local business, with data showing it brought £4M to the region. But in the wake of the event’s economic success, we can’t overlook the many freely-given moments of togetherness and solidarity which form the true backbone of the movement. While the entertainment schedule has evolved over the years, the annual march has remained a constant. And as over 16,500 people showed up in the stifling heat to demonstrate, it’s clear that the procession still proves to be the beating heart of the weekend.
This year, there was a renewed sense of urgency amongst the demonstrators. Palestinian flags were raised high among the usual sea of nylon rainbows and banners, and chants for trans rights were interspersed with calls for liberation beyond our own borders. Celebration walked hand-in-hand with outrage, as children blew whistles to the rhythm of “no borders, no nations, trans liberation”, and many laughed at a hastily-made cardboard sign which proudly announced “my cat is gay”. The crowd burst into dance on Northumberland Street to the tune of the YMCA, then into cries of “shame” as it passed Kings Gate- anger at the institution’s response to the ongoing encampment clearly reverberating across communities.
When I first attended Pride nearly ten years ago, I had less worldly concerns on my mind. At seventeen, I was not joining as a politically engaged member of the community, and I wasn’t old enough to enjoy the dance tents or club wristbands that would later form my typical Pride experience. Having yet to move away from home, it was the sense of freedom that drew me in. We sat on the grass as Belinda Carlisle took the main stage, and I watched with a bittersweet feeling- ‘Heaven is A Place on Earth’ was a family-favourite growing up, played often in our kitchen while tea was cooking on the hob. I thought about those many silly moments, all shared with someone that turned out to be less than accepting of my sexuality. A kind stranger offered to paint a rainbow on my cheek with a Crayola-style stick; it was a cheap and frivolous gift, but I was thrilled at the idea of wearing it for the rest of the day, before wiping it all off on the bus ride home.
I couldn’t help thinking about that stranger as we marched this year, my own crayola-style rainbow stick in my pocket, the faces of friends suitably painted around me. Behind us a brass band played Mama Mia by ABBA, and we danced and chanted along while the currents of the procession made its way past the mostly-cheering onlookers. With the cost-of-living weighing harder on those already experiencing barriers to healthcare and threats to personal safety, it was a relief to feel that the spirit of fun had not been lost- the more sombre sense of commitment I began with quickly turned into excited energy. Perhaps it is in these times of wider struggle that the value of Pride is felt the most, where joy and resistance are two sides of the same coin.
My partner stopped us at one point to wrap a flag around their shoulders, a make-shift shawl of pink, white, and blue. A stranger soon approached to offer a bumble bee, its happy face crocheted in the trans pride colours. It was frivolous, made only for one moment of kindness and fun- in fact there’s likely no problem in the world that can be solved by a crochet bee. But beyond the colourful battalion of the march, we knew well that kindness towards the trans community is an increasingly rare occurrence. When you live something every day, respite is just as necessary as outrage. That small moment of joy had the potential to be a rare gift for someone, and it was one of many that day which revealed that the role of Pride in the community is as important as ever.
When the circuit rounded back to the Civic Centre, there were mumbles of confusion. It seemed that many regular demonstrators were unaware of the drastic change in venue, their attendance at the march guaranteed without the knowledge of ticketed arenas and VIP wristbands. Groups dispersed and scrambled to make their own plans for the day, some disappointed with the abrupt anti-climax, and others eager to explore the new venues and festivities. Amidst the mix of feelings, one thing was abundantly clear while the success of Pride’s event programme continues to ebb and flow with the times, the community’s consistent commitment to Pride sends a powerful message: no matter what happens, we will show up to march.
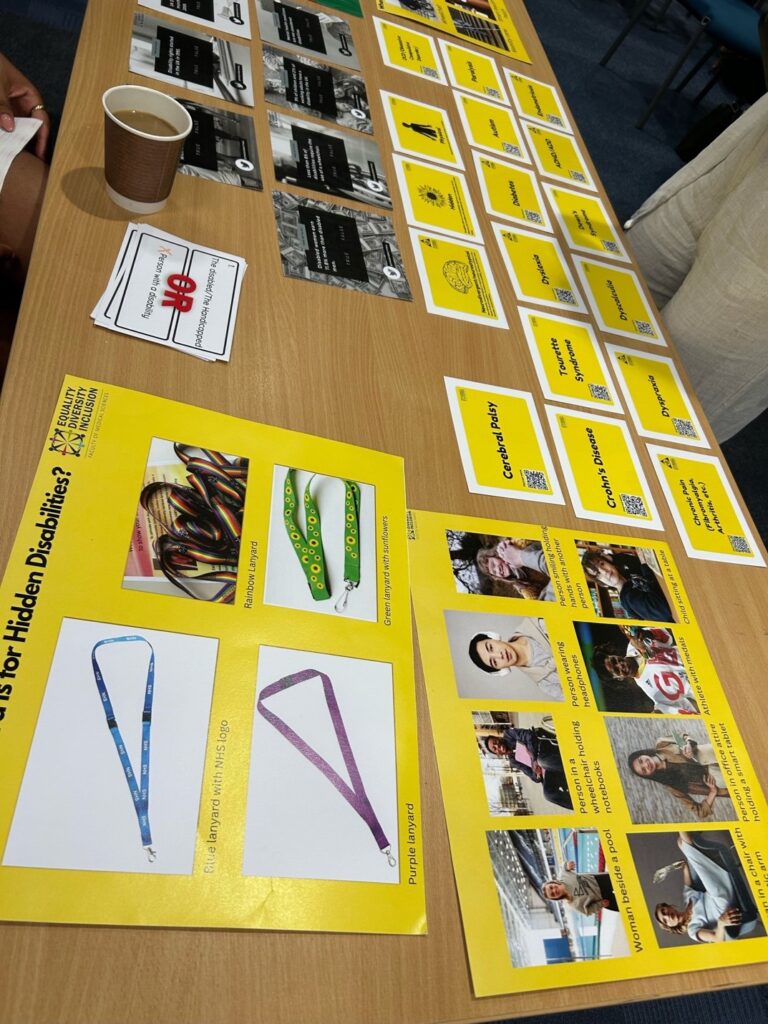
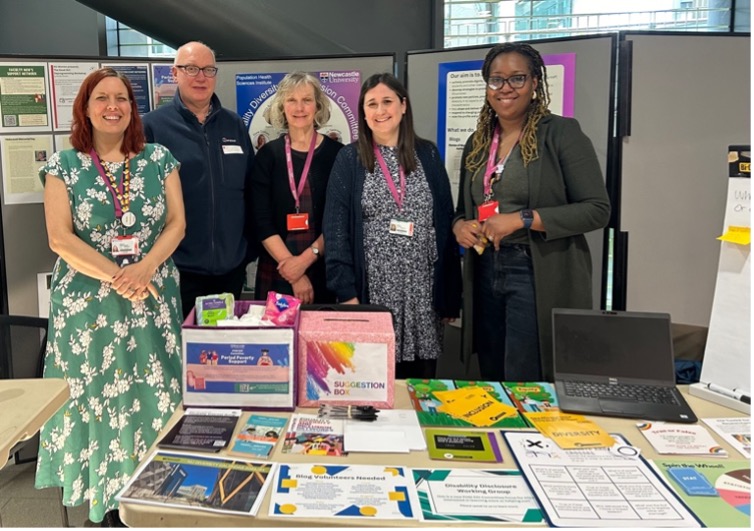
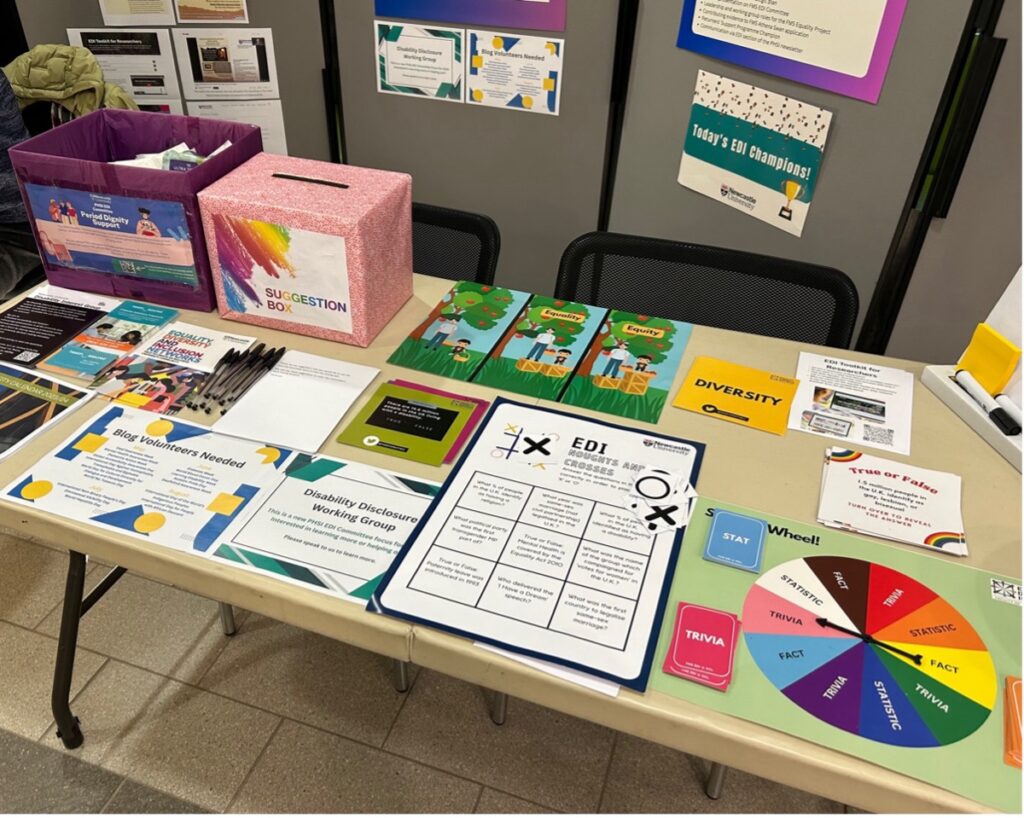
The PHSI-EDI Committee had a presence at the PHSI summer research event on June 25th.
Disability has been flagged as a focus for the Committee this coming year. We are keen to hear your thoughts on tailoring disability support and guidance to best meet the needs of PHSI colleagues. Thanks to all those who contributed their suggestions on the day. If you have any further ideas on how we can expand our disability work or have an interest in supporting this project, please do get in touch: phsi_edi@newcastle.ac.uk
The Committee has also been working on increasing the awareness of disclosure of any disability (both as a staff member or student). Hopefully you will have seen this information in bimonthly PHSI newsletters.
More details can be found below:
Disability disclosure for all colleagues and students at Newcastle University
Newcastle University, including FMS, has fewer disclosures of disability than we would expect to see. Details below on how colleagues can disclose a disability. Sharing information about your disability helps NU work out what changes and support can be offered to you.
Staff processes for informing the university about a disability or long-term health condition can be found here
Students can update their information, including disclosure of disabilities, in S3Pat any time.
Finally, special mention to Connor, Hiruni, Emmie, Ruth, and Viviana for their help on the day setting up and running the stand.
This month, the PHSI EDI committee has been raising awareness of the committee with a stand at the PHSI Spring Celebration Event.
Thanks to all PHSI colleagues who stopped by on April 18th to say hello, to find out more about what we do and how we can help you, or to play one of our EDI games!
Special mention is given to Nicola, Richard, Annette, Ruth, Abisola, and Fiona for running and to Jill, Paul, and Sue for helping to set up the stand.
We had a great turn out and have collected some useful information to inform our onward planning to help develop the committee moving forward.
We will be reflecting on the responses from staff at this event in our next committee meeting and will use any data gained to inform our workstreams moving forward.
If you missed the event or were unable to provide any suggestions on the day. Don’t worry, we are still collating information using an online ‘suggestions box’ (for link, please see the latest PHSI newsletter), so there is still plenty of time to drop the committee a line.
In particular, we are still keen to hear from colleagues who have an interest in:
Getting involved with our blogs.
PGRs who would like to join the committee.
Colleagues with an interest in inputting into the Disability Working Group.
Any other suggestions for PHSI EDI focus this coming year.
Just a few things to recap:
The Committee’s Aims:
Actively promote dignity, respect, inclusivity and equal treatment among staff, students, and other stakeholders.
Develop strategies to promote EDI in PHSI, by engaging staff and students in the process.
Promote new policies, procedures and best practice relating to equality and diversity in all aspects of our activities encompassing all protected characteristics.
Help shape and deliver PHSI EDI culture.
Respond to changing circumstances in PHSI, the wider faculty, and university.
Raise the profile and priority of EDI within PHSI.
What we do:
Bi-monthly EDI updates in the PHSI newsletter – includes links to blogs and upcoming EDI events.
Blogs (linked to themes in Newcastle University’s Inclusion Calendar).
Book Club.
Organise events e.g. online keynote lecture ‘Holocaust Memorial Day & LGBT+ History Month from 2022) – you can still watch the recap online here: https://www.youtube.com/watch?v=CCJQ9mbvM5Q
Period Dignity Project.
Decolonising Research Project.
Disability Awareness Group.
EDI representation on PHSI executive & FMS EDI Committee.
Embed EDI in PHSI strategic plan.
Leadership and working group roles for the FMS Equality Project.
Contribute evidence to the Athena Swan application.
Returner’s Support Program champion.
How we can help you:
Support PHSI colleagues with an interest in EDI – especially those who wish to join the committee (including PGRs).
Promote PHSI colleague’s research by linking this work to Newcastle University’s Inclusion Calendar and EDI themes.
Develop your suggestions for EDI focuses that you would like to see the Committee focus on moving forward.
Ran into an EDI issue? Please contact us to see how we can help you.
February is LGBTQ+ History Month, an annual month-long observance of lesbian, gay, bisexual and transgender history, and the history of the gay rights and related civil rights movements. In this blog, Liam Spencer, Research Assistant in PHSI, reflects upon his research of LGBTQ+ young people’s mental health and experience of attending Stonewall’s LGBTQ+ Leadership Programme .
Liam Spencer is a Research Assistant based at the Population Health Sciences Institute, Newcastle University, and a Mental Health Research Fellow for the NIHR Applied Research Collaboration (ARC) North East and North Cumbria (NENC).
As LGBTQ+ History Month unfolds, it offers us an opportunity to reflect on the strides we’ve made, the challenges we still face, and the incredible diversity within our communities. This month holds particular significance for me – a chance to not only honour the struggles of those who came before us, but also to celebrate the progress we’ve achieved and recommit to the work that lies ahead.
With a background in youth and community work practice, my research interests are primarily focused on children and young people’s mental health, particularly early and preventative interventions, and school-based interventions. My journey as a member of the LGBTQ+ community and as a researcher has been intertwined with a deep sense of purpose – to shed light on the unique mental health challenges faced by LGBTQ+ individuals. This is a mission born out of personal experience, and a desire to contribute meaningfully to the wellbeing of this community. I have recently been involved in several projects funded by the National Institute for Health and Care Research (NIHR) School for Public Health Research (SPHR) Public Mental Health programme, and I’ve had the privilege of being able to delve into the complex dynamics of LGBTQ+ mental health, particularly in school environments. One of these projects, led by Professor Liz McDermott, aimed to investigate the impact of school-based interventions on LGBTQ+ young people’s mental health.
In the first phase of our study, we undertook a realist review (a theory-driven approach) of published evidence and identified positive interventions that supported LGBTQ+ mental health in school environments, however the focus tended to be upon outcomes, and studies rarely detailed underlying mechanistic processes. The second phase of our study aimed to develop a programme theory that explained how, why, for whom, and in what context school-based interventions prevent or reduce mental health problems in LGBTQ+ young people, through participation with key stakeholders.
Interviews were conducted in the UK with LGBTQ+ young people aged between 13 to 18 years attending secondary schools; intervention practitioners; and school staff. A realist retroductive data analysis strategy was employed to identify causal pathways across different interventions that improved mental health outcomes. The programme theory we produced explains how school-based interventions that directly tackle dominant cisgender and heterosexual norms can improve LGBTQ+ pupils’ mental health. Specifically, our theory posits three causal pathways that may improve these outcomes:
Interventions that promote LGBTQ+ visibility and facilitate usualising, school belonging, and recognition.
Interventions for talking and support that develop safety and coping.
Interventions that address institutional school culture (staff training and inclusion polices) that foster school belonging, empowerment, recognition, and safety.
Ultimately, our research underscores the importance of providing a school environment that affirms and normalises LGBTQ+ identities, promotes school safety and belonging, and addresses systemic issues within educational institutions. By implementing evidence-based interventions informed by our programme theory, we can pave the way for improved mental health outcomes for LGBTQ+ pupils.
In August 2023, I won a place on Newcastle University’s ‘Inclusive Futures’ programme – a positive action scheme for under-represented colleagues with protected characteristics to build their skills and knowledge for current and future leadership careers. The scheme is focused on three key areas:
It supports individuals to develop their leadership understanding, skills and networks and encourages participants to consider their career aspirations and goals.
It supports participants’ managers to develop their understanding and skills in being an effective ally and challenges them to reflect on their role to remove barriers and facilitate change.
It creates the opportunity for organisational learning and change by providing spaces for sharing experiences and insights between participants, managers, senior leaders, and decision-makers.
As part of my place on this programme, I also received funding to enrol in an external programme. Recognising the immense value of inclusive leadership in driving positive change, I applied for a place on Stonewall’s LGBTQ+ Leadership Programme, which provides participants with six months of specialist development and support, and I was fortunate enough to secure a spot. In November 2023, I embarked on this transformative journey, by attending a three-day retreat in Buckinghamshire, where I was able to connect with a diverse and impressive array of individuals, and hone my skills as an advocate and future leader.
This month serves as a powerful reminder of our collective resilience, our shared struggles, and our unwavering commitment to justice and equality. Let us continue to push boundaries, challenge norms, and advocate for a world where difference is celebrated and all are embraced for who they are – within academia, our personal lives, and beyond.
This blog was written by Annette Pantall, Lecturer and NUPHSI EDI Representative for the Neuroscience, Neurodisability and Neurological Disorders research theme.
Dr Annette Pantall, Lecturer Neuroscience
Holocaust Memorial Day (HMD) took place on 27th January, the anniversary of the liberation of Auschwitz-Birkenau concentration and extermination camp. HMD is commemorated by events locally as well as nationally and internationally. Local events included the Brundibár Arts Festival held in Newcastle and Gateshead, featuring music written during the holocaust. HMD remembers the 6 million Jews murdered during the Holocaust together with millions of other victims of Nazi persecution. Over 200,000 Roma and Sinti people and other groups who did not fit in the Nazi ideology of racial purity including disabled people, gay people, political opponents, and various religions were murdered. Additionally, there are those whose lives were never lived due to forced sterilisations. The importance of this day therefore extends far beyond the Jewish community and is relevant to all, whatever their religion, race, ethnic background, politics, or sexual identity. Stone wall former chief executive, Ben Summerskill, explains why HMD is an important day in the Equalities calendar. The Nazis forced people identified as gay to wear an inverted pink triangle – ‘die Rosa-Winkel’ – like the yellow star of David Jewish people were compelled to wear. HMD emphasises the importance of maintaining the principles of equality, diversity and inclusion to prevent antisemitism and other forms of prejudice, intolerance and hatred which resulted in the horrors of the Shoah (Hebrew – catastrophe).
Relevant to us, working in FMS at Newcastle, is the role of teams of medical doctors and researchers in the Nazi genocide program. In 1939 the killing of disabled children and adults started which required a panel of medical experts to give their approval for the killing of each child. This extended to adults with chronic illnesses, disabilities, and mental health problems. In total 250,000 disabled people were killed, and 6 extermination camps were specifically set up for this purpose. It has been estimated that 250,000 people diagnosed with schizophrenia were murdered or underwent forced sterilisation. Between 1939 -1945 Nazi physicians were involved in 348 coerced medical tests performed on a total of 27,761 people. Many of the physicians and researchers were never prosecuted.
In addition to the 6 million Jews and other groups murdered by the Nazis, HMD commemorates more recent genocides in Cambodia, Rwanda, Bosnia and Darfur. Many more genocides could be added including the persecution and murder of Rohingya Muslims or the 1915 Armenian genocide. England has also had its share of genocides and persecuting minorities. In York on 16 March 1190 the entire Jewish community in York was massacred in Clifford Tower. In 1645-46 in East Anglia, over 300 women who did not fit in with the female norm were deemed witches and killed by the ‘Witchmaster General’ Matthew Hopkins. In the 1930’s Oswald Mosely formed the British Union of Fascists, which became increasingly antisemitic but was eventually banned by the Government.
This year’s HMD’s theme is ‘Fragility of Freedom’ reflecting the escalating anti-Jewish legislation introduced by the Nazis which increasingly restricted civil rights for the Jewish people. Initially they were excluded from certain professions and schools and universities. The draconian Nuremberg Laws were introduced in 1935 curtailing freedom of the right to marry and defined a Jew based on the number of Jewish grandparents. The restrictions of freedom form part of the ten stages of genocide and culminated in the murder of over 6 million people Jewish men, women and children which represented two-thirds of Europe’s Jewish population.
Soon there will no more survivors of the concentration camps, the Warsaw ghetto, victims of experiments and sterilisations to provide us with those shocking first-hand accounts. An old family friend, Paul Porgess, who as a child survived the Warsaw Ghetto, died last April. Seeing and talking to Paul who lived during those unimaginable terrors makes it real. The danger is that when there are no more survivors the Shoah will become history, a story from the past with the horror so intense that it is almost impossible to comprehend. As George Santayana reminds us “Those who forget the past are condemned to repeat it”. However, remembering alone as Auschwitz survivor Anita Lasker Wallfisch stated, is not sufficient – ‘you remember on the 27th but forget on the 28th’. Instead, an understanding of why these events developed must be considered.
During the virtual 2021 Holocaust Memorial Event Anita Lasker Wallfisch in her concluding comments emphasised the importance of being curious about Jewish people and their history and customs. Without knowing about different customs – for example what is Kosher food (and why is it not available at Newcastle University?) or what are the laws governing Shabbat – prejudices and alienation can develop. The North-East has a thriving Orthodox community in Gateshead which was described by a New York Rabbi in the Guardian in 2019 as the ‘Oxbridge of the UK Jewish community’. Yet how many of us at Newcastle University know that we have this on our doorstep? Similarly, regarding other faiths, how many know about the Halal food laws, the month of Ramadan or requirements of Muslim men to attend prayers on Fridays? Understanding and knowledge of other groups is essential for inclusion.
The poem by Pastor Martin Niemöller ‘First they came’ summarises why one should commemorate HMD and be actively involved in EDI issues.
December 3rd 2023 markedInternational Day of Persons with Disabilities. This date is celebrated annually, serving as a reminder of the need to promote both an understanding and awareness around disability issues and the well-being of persons with disabilities.
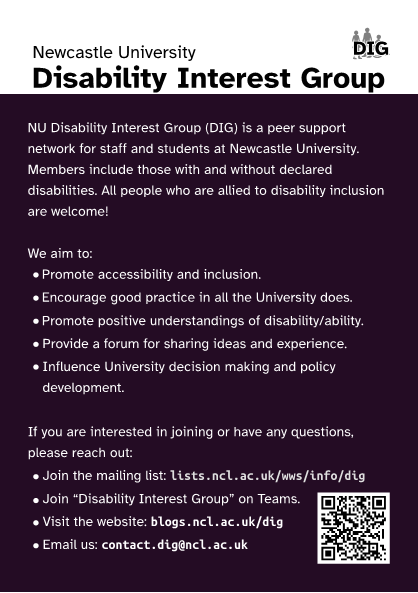
This month we caught up with Newcastle University’s Disability Interest Group (DIG) to find out more about disability inclusion in academic life.
What is Disability?
Disability is defined as a physical or mental impairment that has substantial, long-term (at least 12 months) adverse effects on a person’s ability to carry out normal day-to-day activities. The scope of disability is wide and can change with time. Disability examples include: neurodiversities (e.g. autism, dyslexia); mental health conditions (e.g. depression, anxiety) and; physical health conditions (e.g. sight loss/vision impairment, chronic fatigue syndrome). Many disabilities are not visible.
Law Around Reasonable Adjustment
The Equality Act 2010 outlines when someone is considered to be disabled and therefore protected from discrimination. It stipulates the ‘reasonable adjustments’ (e.g. policy changes, working practices, physical layout alterations or provision of additional equipment) that employers are required to make (and pay for) to ensure that people with disabilities are supported in their workplace. Failure of the employer to comply to the Act is a considered a form of discrimination.
Any adjustments which will benefit all individuals, not just those persons with disabilities, should always be advocated for. For example, clear signage in university building and provision of meeting agendas well in advance benefits everyone.
Work based adjustments are available for both PGR students and staff members.
Employee Entitlements & Further Resources
To find out more and to check what support you may be entitled to, the following resources may help:
DIG are always open to expanding their network and welcome anyone wishing to join their community.
Information in this blog post was complied by Ruth Norris, Research Associate
Finally, as we all gear up for the University’s closure over the festive period, one action we can all take regarding caring for our mental health is to encourage a healthy work/life balance. So, take a break, recharge, and come back afresh for 2024.
We look forwarding to welcoming you back in the New Year!
This year, UK Disability History Month (UKDHM) focuses on the experience of disablement amongst children and young people in the past, now and what is needed for the future to reduce the stigma, stereotypes, negative attitudes and socially created barriers in the environment and the way things are organised.
Dr Sarah Wigham, Senior Research Associate
To mark UK disability history month, we caught up with colleagues Sarah Wigham (Senior RA) and Simon Hackett (Clinical Senior Lecturer) to find out more about their research about improving access to healthcare for people with Learning Disabilities.
Dr Simon Hackett, Clinical Senior Lecturer
What is the focus of your research?
Our research projects focus on the health care and health needs of people with a learning disability. People with a learning disability experience high levels of inequality in their health and marginalisation in access to health care services compared with the general population. Our research aims to develop resources that may help to reduce some of these barriers and inequalities.
One area of our work focused on how barriers that people with a learning disability face accessing primary care could be removed. We worked with people with a learning disability to create ten recommendations to make accessing the doctor’s surgery easier for people with a learning disability.
Why do you think this research is important?
Research has shown that people with a learning disability die much younger than the general population. The average age of death for people with a learning disability is 61 years compared with 81 years in the general population (LeDeR, 2018). They have more mental and physical health problems and more problems accessing health services.
Many people with a learning disability are prescribed medication. A key aim of the UK Government NHS Long Term Plan is to improve understanding the health needs of people with a learning disability and reduce use of medication for people with learning disabilities.
What are the main challenges?
Primary healthcare systems may not be accessible for people with a learning disability. For example, people with a learning disability may have problems using the telephone appointment system. Annual health checks which are carried out by general practitioners (GPs) and nurses can help to identify health problems and address health inequalities experienced by people with a learning disability. However, our research shows that primary care systems are organised in ways that can create barriers and make it difficult for people with a learning disability to access.
We also found that there are barriers to the identification of mental health conditions among people with a learning disability in primary care.
What are the biggest opportunities to reduce the stigma around disabilities?
We published our findings from a recent study in the British Medical Journal Open and we hope that lots of nurses and doctors working in primary care will read the article and that it will help improve access to primary care for people with a learning disability. You can find out more about our work on improving access to primary care for people with a learning disability in recent outputs:
To launch the new NU Diversity Calendar this September, the PHSI EDI committee is marking International Day of Sign Languages on the 23rd of the month. This special date commemorates the establishment of the World Federation of the Deaf in 1951 and aims to promote the celebration of linguistic equality, diversity, and cultural understanding.
Worldwide, there are more than 70 million Deaf people who collectively use more than 300 different sign languages (a language which conveys meaning visually with hands, facial expressions, and body language). Historically, sign languages have faced limited recognition and acknowledgement as official languages. The International Day of Sign Languages provides an opportunity to address these concerns through celebrating and raising awareness of the importance of sign languages in the human rights of those who are Deaf.
The theme for this year’s International Day of Sign Languages is: a world where Deaf people everywhere can sign anywhere. To mark the day, two colleagues (Niamh Foy and Sally Lamond) from the School of Education, Communication, and Language Sciences (Faculty of Humanities and Social Sciences, HAAS) share their thoughts on sign language inclusivity.
Sally Lamond, MSc Language Pathology Student
A Culture of Compassion
What is the International Day of Sign Languages?
Established in 2017, the International Day of Sign Languages is celebrated annually on the 23rd September. It’s a day for celebrating the wonderful diversity of language needs, raising awareness of the rights and struggles of individuals who use sign languages to communicate.
In an era where a quick google search can reveal important dates such as “Talk like a pirate day” (19th September, for the curious) or “International Beer and Pizza Day” (9th October, if you are so inclined to save the date), it seems clearer than ever that amidst the backdrop of innumerable “International” days, this is one that is deserving of some more attention.
What is sign language?
Whilst most individuals outside of the signing community are likely aware that sign language uses visuals (hand shapes, facial expression, and body language), many may be unaware of the high variation and nuance of signing. Far from being internationally mutually intelligible, “sign language” comes in many “shapes and sizes”; wherever humans exist, language exists, and wherever deaf, Deaf, Hard of Hearing (HoH) (DHH) or otherwise non-verbal individuals exist, sign language will inevitably evolve to fulfil the human drive for connection and communication. Whilst here in Britain we use British Sign Language (BSL), our friends across the pond use American Sign Language (ASL), those in New Zealand use, perhaps unsurprisingly, New Zealand Sign Language (NZSL)…and so on. Despite these varieties often being unique to a country or region, sign languages are not, as some might speculate, verbatim “translations” of spoken language either— they consist of distinct vocabulary, connotations, and complex grammar unique to them.
Signing as an Alternative and Augmentative Communication (AAC) method
Whilst many signing systems are fully fledged languages in their own right, as a Speech and Language Therapy student, it would be remiss of me not to mention the versatility of sign as an AAC technique, however briefly. Makaton, a simplified signing system based on BSL and developed in the 1970s by a team of Speech Therapists, is a prime example. The signing system was created by selecting and altering core BSL concepts for use with children and individuals with learning disabilities; these signs are used in conjunction with speech to support communication. These individuals, who may be unable to express themselves verbally or who may struggle to understand spoken language, can be supported by learning meaningful, consistent gestures.
In the decades since, the system has become increasingly popular in early years and additional needs settings, and becoming certified has become exponentially more feasible for many as courses have spread across the country. Though true Makaton proficiency is measured in levels 1-4, the internet is a fantastic resource for exploring some of these simple signs— and as a matter of fact, the Newcastle University Speech and Language Therapy Society engages in “Makaton Mondays”, where a weekly Makaton sign is shared.
Why is sign language awareness important?
In brainstorming this blog post, I was prompted to consider my own awareness of sign language. I vividly remember the first time I— 17 years old at the time, and in the first of many customer service roles I have occupied in the decade since— served a signing customer. Despite being born in the UK and using a language with “British” in the title, I was faced with the reality that this individual likely experienced daily frustration and accessibility issues I would never have to, largely due to others’ lack of knowledge and (to some extent) lack of effort. Put simply, it felt unfair, and I was embarrassed not only by my own lack of signing ability, but by my lack of awareness of the lack. The realisation was disconcerting, suggesting a key question: what exactly is our level of responsibility to each other in this domain?
Years (and several encounters with signing customers) later, I finally embarked upon an introductory sign language course in an effort to bridge the gap I had become aware of (which, of course, served to humble me further— I’ll reiterate here that sign languages have their own grammatical rules). I was very fortunate to do so through a local university society; though the course itself was self-funded, the university subsidisation made it feasible and affordable in a way many BSL courses simply are not.
As Language Pathology/Speech and Language Therapy Students, we are taught repeatedly that everyone has a right to a voice, and that every voice matters. The right and ability to share one’s hopes, dreams, opinions, and experiences is intrinsically tied to the autonomy every person innately deserves. To this day, I think admiringly of the patience and grace signing individuals must cultivate simply to exist in a linguistic environment which, at best, frequently overlooks them and at worst, is actively discriminatory and unwelcoming.
Cultural impact
As cultural awareness of sign languages has grown in recent years, they have begun to be seen not only as a communicative tool for those who are unable to produce or understand spoken language, or for those may be non-verbal for other reasons, but as living, breathing languages which can be equally— if not more— expressive than spoken languages. We do not have to look very far to see examples of incredible DHH signing individuals who are turning the tide of public perception, showing the rich diversity and creativity within the signing community. ASL interpreter Justina Miles, for example, who took the world by storm with her sign performance at Rihanna’s Superbowl halftime show earlier this year, ultimately going viral across multiple social media platforms as she brought the music alive for Deaf and hearing viewers alike.
The concept of sign performing, as opposed to traditional interpretation, allows sign language users greater access not just to the verbal content being expressed but opens up the door to the attitude, the atmosphere, and to being included in the collective enjoyment of fellow fans. This is relevant to all ages, as is evidenced by the recent creation of SignUp captions (www.signupcaptions.com), a chrome extension which provides access to Disney movies for younger viewers through sign performance—current supported titles include hits such as Frozen, Moana, and Encanto.
With the rise of social media which centres around videos (such as Instagram and TikTok), members of the signing community are also joining in the creation of content which details the huge spectrum of DHH experience; ranging from joy and pride to struggles with accessibility and discrimination. Content creators such as Estefani Arevalo (@thatdeaffamily), Janet Moreno (@deafmotherhood), Felicia Aquilo (@feliciaaquilio), Beth Leipholtz (@beth_and_coop), Brittney Nolte (@brittneynoltee) are sharing the realities of raising children in the Deaf community, both as hearing and Deaf parents themselves, with discussions relating to Cochlear Implants (CI), views on “passing” the newborn hearing test, and tips on making sign learning fun for toddlers. Younger creators are being empowered to share their experiences through sign— for example, Savannah Dahan (@savvyasl) a 13-year-old who has recently become the first Deaf KidzBop performer and speaks about wearing hearing aids, or Kylee (@tjandkylee), a young girl who raises awareness of hearing loss through making informative and entertaining videos with her dad, TJ. Deaf teen TikToker Elizabeth Harris (@lizzytharris) and Child of Deaf Adults (CODA) Jon (@drunkcrier) are also well-known influencers in the space.
A ways to go…
Though public awareness of sign language is growing and perspective shifting, there is still much room for improvement. Consider this challenge: as you go through your daily activities, think about whether they would be quite as accessible to you, were you a sign language user. Getting a ticket for the bus, ordering your morning coffee, metro announcements; there are work arounds, of course, humans are nothing if not adaptable. But my question is this— why should the DHH community have to accommodate hearing individuals quite so extensively? What compromises can we collectively make to ensure that accessibility is not an afterthought, but at the core of design?
Is it reasonable to expect that every UK citizen will become fluent or bilingual in BSL? Well, no, of course not. Is it unreasonable, however, to suggest that some core signs be taught in schools alongside the standard Spanish and French? My answer would have to be the same— of course not. Compassion and access to participation should not be a luxury.
Niamh Foy, BSc (Hons) Human Communication Graduate
The Quiet Stigma Around Silence
As a society, we have a problem with silence. Namely, the fact that we can’t decide whether we like it or not. In English, we only have to look at the rich tradition of idioms related to silence to grasp the outline of our complicated relationship with it. Silence can be eloquent, stony, or heavy; for some it is golden, and for others, it is paradoxically ‘deafening’. We can listen to radio silence, or be part of the silent majority. Silence can be physical – irreparably damaged when we ‘break our silence’, or crashed into, like a ‘wall of silence’ after an awful work presentation. We can give birth to silence with a pregnant pause, or, ominously, be as silent as the grave. Some people even choose to administer silence like a medication, by giving loved ones or friends ‘the silent treatment’. And if that’s not enough, we may find ourselves facing a ‘silent killer’ when we carry a disease with no obvious symptoms. It’s enough to make anyone want to stay quiet.
I think there’s a reason for our fascination with silence, and it relates to two key desires of human beings; we are natural born communicators, and we are also helplessly self-interested. We naturally want to forge bonds with others through shared stories, confessions, and conversations – and even better if these dialogues concern our own hobbies, interests, and welfare needs. Silence, which by its nature is nonverbal and is indifferent to all parties, flies in the face of both of these desires – and that can be a shock to the system for many. There’s something wonderfully human about the fact we have a word for when we’re not talking.
In the speech and language therapy community, we face the same confusion regarding silence as the wider culture, but in ways which are technical rather than literate and much more pressing given the impact that our work has on real life human beings. Speech is the raw material of a speech and language therapist – like a carpenter’s timber, a blacksmith’s iron or a farmer’s wheat. And yet, there is growing dissent against the notion of ‘oralism’ within the speech and language therapy community; the belief held by some members of the profession (perhaps subconsciously) that speech is the be-all-and-end-all, and that other methods of communication such as sign languages, writing, and gesture are comparably inferior.
Pushback against oralism is felt acutely in the Augmentative and Alternative Communication (AAC) community. AAC refers to any type of artificially added (augmentative) communication method used instead of (alternative) speech. AAC can be high-tech, with iPad-like Voice Output Communication Aids, or low-tech, with clients using specially-made picture books and cards to help get the message across. Famous AAC users who have pioneered AAC in mainstream media include the late physicist Stephen Hawking, ‘Britain’s Got Talent’ comedian Lee Ridley, rugby league hero Rob Burrow, and cerebral palsy activist and blogger Beth Moulam. Whilst these four individuals are much-appreciated trailblazers, a great deal of further work and investment is needed to promote the views and welfare of AAC users in daily life. Anyone who has worked alongside a speech and language therapist in their practice, or anyone with a loved one who uses AAC, will be all too familiar with ‘horror stories’ around maltreatment of AAC devices by carers, teachers, and healthcare workers – communication books being left out of reach of a client in a hospital bed; children’s Voice Output iPads being smashed, left to drain their battery, or even locked away in cupboards while at school; confused clients being handed AAC without proper guidance or modelling of how to use it. All of these experiences are rooted in a pervading and unwelcome societal preoccupation with oralism. Since the AAC device is seen as inferior, it is given less respect and decency than a person’s spoken voice. But an AAC device may well be a person’s only way to communicate – would you tear out a person’s larynx and leave it in a cupboard, or lock someone’s mouth shut and leave the key painfully out of reach?
I write with feverish discontent about this issue because I myself have some experience of having my voice locked away without my consent. As a child I experienced what is now called ‘situational mutism’ but was then called ‘selective mutism’ – a medical speech disorder caused by uncontrollable anxiety, where the speech functions shut down in seemingly innocuous but underlyingly stressful situations. This meant that I barely spoke outside of my house for the first ten years of my life, mainly relying on a faint knowledge of British Sign Language (BSL) and a lot of gesture to get my message across. Whilst I did have a few friends in school, I was bullied, and retreated into a world of creative writing and drawing to express my feelings. One of my most bittersweet childhood memories is telling my favourite teaching assistant that I had a new little brother by drawing a pencil sketch of a baby on some green paper she had salvaged from a cupboard. That little baby is now a strapping lad of sixteen and is probably taller than me and the teaching assistant combined, but that memory is as warm as my love for him. To the ardent oralist, this memory is indicative of failure, since I wasn’t able to use my voice to tell this teaching assistant my thrilling news. But to me, this moment remains as a touching example of tenacity and creative ingenuity from two different people in the face of a communicative challenge.
There are some individuals who place a special amount of virtue on silence and mutism, to the point of viewing silent contemplation as a necessity for spiritual discernment. As a Catholic, I find myself drawn to the example of St Benedict of Nursia, the Patron Saint of Europe known for his demon-fighting medals and for sharing his name with sixteen Popes. St Benedict was born into a noble family, but after witnessing the vices his fellow rich students indulged in and the political situation in Rome, decided to run away and live in a cave (increasingly tempting in today’s world … ). To this day, the Trappist monks inspired by St Benedict spend most of their daily lives in silence in order to better receive the will of God, and have even developed their own ‘monastic sign languages’ to communicate in the monastery. Whilst these monks took silence to the next level, even lay people have a natural understanding that quiet contemplation can unlock secrets which idle chatter cannot. How many of us meditate, pray, or need perfect silence to sleep or study?
In this blog post, I’ve touched upon two communication needs discussed in the speech and language therapy community – AAC and selective / situational mutism. However, there are plenty of examples of other areas of speech and language therapy where negative attitudes and stigma about alternate communication methods act as a barrier for clients and clinicians; speech and language therapist (SLTs) working in care homes and in the community with adults living with dementia, SLTs working with adolescents and adults with learning disabilities, and SLTs working with young offenders in the criminal justice system spring immediately to mind.
If you enjoyed this blog post, I’d highly recommend delving into the writings and work of some speech and language therapists and academics who have addressed this issue before me: Dr Helen Robinson, who specialises in AAC and is the Royal College of Speech and Language Therapists’ representative for the North of England; Warda Farah, an entrepreneur and lecturer at the University of Greenwich; and Professor Pam Enderby OBE, who has worked for over 40 years with adults living with conditions such as dysarthria and dysphagia, and is lovingly referred to by some as the ‘rockstar’ of speech and language therapy. I’d also like to thank the Selective Mutism Clinical Excellence Network (CEN) who made me feel really welcome when I was reflecting on how best to approach this blog.
This International Day of Sign Languages, I’d invite you, the reader, to reflect on your own experiences of alternate communication methods – have you observed attitudes of oralism out in the world, or unwittingly pushed them yourself? What is your favourite method of communication besides spoken language? Do you know anyone with a speech, language, and / or communication need? What will you take forward from today? And, if you’ll pardon the pun, what communication inequalities are you willing to speak out about?
Mental Health Awareness Week runs from 15 to 21 May 2023. In this blog, PHSI colleagues Dan Steward, Emily Oliver, Fiona Duncan and Ilaria Pina, tell us more about their mental health research and experience of working in this area.
Dan Steward, Research Assistant
What is the focus of your research?
We are a team of researchers working on the promotion of positive mental health, and how best we can support thriving, rather than just ‘surviving’, for all. We try to explore new and creative ways to provide support, drawing on different ways of thinking about what it means to be mentally healthy as well as diversifying who is involved in providing support.
An individual living with a severe mental illness (SMI) dies on average 15-20 years earlier than someone without an SMI, and health inequalities continue to worsen in the Northeast of England. Currently, our main project is focused on improving the lives of people living with SMI in Northeast England. The WHOLE-SMI project explores holistic approaches to health and supporting people to live well, with a focus on how best we can embed physical health promotion services within support pathways for people living with SMI.
Another area of work is centred around whether and how community organisations can use digital technology to promote good mental health and wellbeing, reduce social isolation and loneliness and prevent mental illness. Crucially we will investigate which groups in the community are more or less likely to benefit from using digital services.
Emily Oliver, Professor of Behavioural Sciences
How did you get involved in this area of research?
Our team have diverse disciplinary, theoretical, methodological and prior research backgrounds, but with a common goal of improving physical and/or mental health and wellbeing. Collectively, we have worked with cohorts ranging from those living with severe mental illness, overweight and obesity, individuals living with prediabetes, our older populations, staff within the NHS, people living in lower-middle-income countries, and professionals working in elite performance environments. We became involved in this work as we feel particularly passionate about addressing the challenges that face people living with SMI or other complex circumstances, and we all feel very strongly that more needs to be done to help everyone to live healthier and longer lives.
Why do you think this research is important?
The facts and figures speak for themselves, particularly when it comes to life expectancy and SMI. There is also still a large stigma associated with mental illness and we all advocate breaking this stigma to facilitate individuals to experience better quality of life and live longer. We recognise that current service delivery has a tendency to be compartmentalised and not address the whole-health needs of an individual, especially when there may be underlying causes affecting other aspects of a person’s health that are not acknowledged. We have found that there is an appetite for a change of approach to health from stakeholders and patients alike. Additionally, we respect the different burdens our primary, secondary and community care providers face. We understand the importance of facilitating service delivery as effectively and efficiently as possible.
Fiona Duncan, Research Associate
What are the main challenges?
As with all research, we have also experienced challenges in our studies. A challenge we have faced in recruiting experts with lived experience has been developing new ways to support the involvement of groups that are typically underrepresented in research. For example, we have recently engaged with a charity organisation called The Lawnmowers Independent Theatre Company, run by and for people with learning difficulties, who have helped us better understand their experiences with research and how we can be more approachable and accessible to potential participants in this demographic. We have also experienced challenges with competing priorities and demands, not just within our own workloads, but also that of the healthcare professionals we have engaged with. With services stretched, we have found having conversations with healthcare staff via existing NHS structures (e.g., team meetings or training sessions) and attending clinics and sites in person for short data collections ‘on the hoof’ to be helpful.
Ilaria Pina, Research Associate
What are the biggest opportunities to reduce the stigma around mental health?
Communication and engagement! Whilst massive improvements have been made in how we discuss mental health, there is still a long way to go. Additionally, we need to consider those that have been brought up to mask their feelings and how we change the conversation to include them and help them more. In doing the research we do, we have a heightened appreciation of the importance of listening to the experiences, opinions and needs of those in the community, those with lived experience of having an SMI, and those on the front-line delivering vital services and support. As Dan in our team says, “I think the biggest opportunities to reduce the stigma around mental health are in the open and two-way conversations we have with people, and sharing our experiences, whilst also being open to changing how we approach mental health.”
Easter is one of the most important festival in the Christian calendar. The date of Easter Sunday varies from year to year. It is celebrated on the first Sunday after the full moon, on or after 21 March. This year Easter Sunday falls upon the 9th April 2023. PHSI Research Associate Dr Abisola Balogun-Katung shares her reflections of Easter celebrations past and present.
Easter is one of the biggest festivals for the Christian church. It is when the resurrection of Jesus Christ on the third day after his crucifixion is celebrated. In more modern times it has become a celebration that everyone regardless of their religious affiliations or beliefs can partake in. Though the origin of the word ‘Easter’ is uncertain, a school of thought is that it is derived from the Anglo-Saxon goddess of spring and fertility, Eostre, whose animal symbol is a bunny. Celebrated with family and friends, Easter Sunday lunches, egg hunts, bunnies this mix of pagan and Christian traditions (and a whole lot of commercialisation), has become one of the most exciting traditions in the UK.
I reminisce about how Easter was celebrated growing up in my hometown Lagos, a multi-cultural and -religious a city with a large population of Christians. The Easter festivities commence with Good Friday, the day Jesus Christ was crucified. This prelude to the Easter celebrations is a solemn day of deep reflection and introspection. In some areas of the city, it would be common to see re-enactments of the process to the cross and the final hours of Jesus’ life played out on the streets. Men dressed in Roman military clothing, holding swords and whips, hurling curses, and walking behind a man carrying a huge cross, donned with a purple seamless robe and a crown of thorns. They would make this journey round the streets as onlookers would shake their head in pity and some even weep. Some who observe this day, fast, and abstain from dairy foods and beef, pork and goat meat. We would have neighbours bring Frejon, a local delicacy enjoyed by emancipated Nigerian returnees from Brazil who settled in Lagos after the abolition of the slave trade, a story for another blogpost. I can almost taste the delicious and flavourful thick pudding made with coconut milk and beans usually accompanied with fried peppered fish or snails.
The next big event following Good Friday is on Sunday, Easter Sunday. The long-awaited day for many Christian adherents, the day of Christ’s resurrection! There would usually be a church service held and people would celebrate the great resurrection after three days. The joy and happiness, palpable! After the 4-hour church service, yes, 4 hours! We would be dismissed by the preacher to our homes. My family and I would drive to my Aunty Abosede’s house, now Aunty Abosede made the best Easter Sunday lunch, the roasted whole chicken, jollof rice and golden yellow plantains fried to perfection. I always looked forward to that. The parents would sit in the living room, chatting about the latest news, while the children played hide and seek or noughts and crosses.
I recall one Easter, the church across the street from my family house having an outdoor procession, jubilating, dancing and shouting, ‘He is risen’. This is how Easter Sunday was typically celebrated. The following day, Easter Monday, the wrap up to the long weekend. For those who had not had enough of the Easter Sunday festivities, they carried on into the night not minding they had to wake up in time for work the next morning. Music blaring, drinks, and food flowing endlessly. For others, like myself, it was a day of relaxation, perched on a chair, enjoying the cool mid-day breeze on my face, and getting lost in my thoughts.
Easter this year, for me would be a little different. I intend to spend it relaxing at home with my family in Newcastle. I will attend my local church service on Sunday and join in with friends to enjoy the North East cuisine. For me, it will be a time to reflect and recharge. No matter how you choose to spend Easter, with family, friends or alone, with a book, in bed or at an Easter egg hunt, make sure you spend it doing at least one thing that brings you joy. Have a lovely Easter Break.