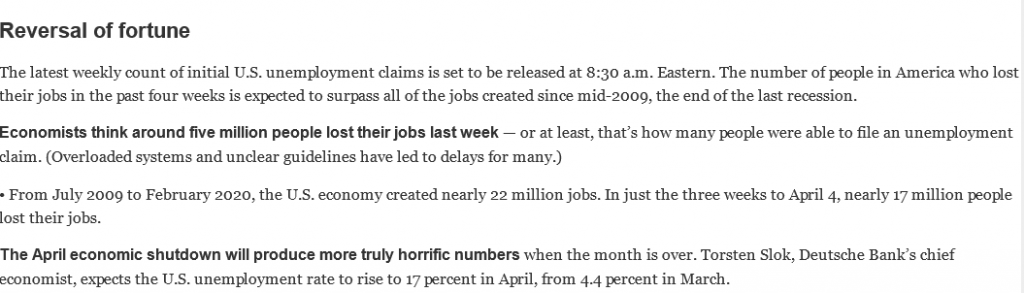
I have previously mentioned Andrew Sorkin’s DealBook blog, which I regard as indispensable. Here’s an example: The first paragraphs of today’s (16 April) update about the situation in the United States:
Think about the short- and long-term health implications of that last figure, and the situation in many other countries, which will no doubt be comparable. If you take the social determinants of health inequalities at all seriously, you can’t ignore them, even though too many of my colleagues would prefer to do so.
Herewith a
few equity- and policy-oriented musings about the latest state of the pandemic
world.
1. Media, and many researchers who should know better, seem obsessed with the number of deaths from Covid-19, or associated with Covid-19. Good reasons exist to want to know this over the short term, for purposes of tracking the spread of the virus, but apart from the fact that in most countries the current chaos makes it impossible accurately to determine this number, it is largely irrelevant in terms of the overall health impacts of the pandemic.
The most basic indicator that matters is the all-cause mortality rate (age-adjusted or not, and both figures should be presented), and the inequalities in this indicator amongst various age, class, gender, race/ethnicity and regional demographics. Over time, all-cause mortality rates will reflect not only the short-term health system dislocations and dysfunctions associated with the pandemic, but also the longer-term impacts on social determinants of health of the depression that will follow the lockdown. In a few years, those of us still alive will be able to compare the effectiveness of various national responses … and to restate a point it is all-cause mortality, and not the number of deaths directly attributable to Covid-19 or among people tested positive, that matters. Dead is dead, whatever the cause.
2. In the UK, I continue to be baffled by the utter lack of comprehension among people professing a concern for equity of what economic downturns of the magnitude now apparently envisioned by Treasury – and of course these anticipations are all dependent on the assumed length of the lockdown, the nature of the exit strategy, and the economy’s subsequent response – will mean for everyday life and for the economic substrates of health inequalities. The cynical me suspects that most people in a position to prognosticate with anyone paying attention have gardens and can comfortably work from home, unlike much of the rest of the population.
Let me suggest just one example of probable impacts:
Concern about the fate of high street commerce has long been unmatched by meaningful policy response. Mr. and Mrs. Range Rover, who matter most in political terms, usually shop online or in the suburbs. Post-pandemic, for hard financial reasons, it is likely that local authorities will simply cease providing services to low-occupancy commercial high streets, and utilities will be released from whatever obligations they have to provide services in those areas. There will be few users, and fewer still who are able to pay their bills or council taxes.
A fantasy? Not at all. A variant of this policy was partially adopted as “planned shrinkage” in New York City in the 1980s, and much more recently in post-bankruptcy Detroit. There will be no-go high street wastelands of abandonment, at least until some far distant future when they will become attractive for reinvestment (beyond the lifetimes of many of us).
Alternatives can be imagined, in abundance (and will be the topic of a future post), but it is hard to think that any UK government will pursue them in the near future, especially as the country’s post-pandemic economic policy may well be managed jointly by the International Monetary Fund, as gatekeeper, and China, as the only external actor with the resources necessary to provide direct investment on the scale necessary.
3. Even if the UK’s post-Brexit departure from the single market and customs union is delayed, as it should be, the full scope of the dislocations will become clear at the start of next winter, when it becomes clear how many Britons simply cannot afford to heat their homes. Watch the all-cause mortality rate carefully as that happens.
Like many colleagues, I have spent the past decade and a half mainly investigating the way in which macro-scale economic and social conditions and policies affect health by way of the unequal distribution of exposures, vulnerabilities and opportunities – the social determinants of health. The way in which authorities in the UK and elsewhere have responded to the coronavirus pandemic cries out for analysis from this perspective. Yet most colleagues’ silence has been deafening. Why?
After all,
to stay with the UK situation for the moment, the best post-pandemic outcome
that can be anticipated is a prolonged recession, the consequences of which
will be distributed unequally. Despite
temporary assistance, many small businesses will not reopen, and many workers
will exhaust temporary supports as their employers fail. After a decade of austerity local authorities
are, to put it mildly, ill situated to provide necessary assistance. Such predictions are necessarily cast in
general terms. Modelling the behaviour
of economies is even more difficult than modelling epidemics of communicable
disease, not least because external influences outside the control of even the
best intentioned national policy-makers are more significant. Yet the population health community in the UK
has been almost completely silent on these issues.
I suspect that part of the answer has to do with apprehensions about being identified with arguments for cautiously restarting the economy that mainly originate from the political right, like Gerard Lyons’ piece in The Telegraph or President Trump’s (in)famous statement that the cure cannot be worse than the disease – which, taken at face value without regard for its deranged originator, is unexceptionable. In the political arena, such an apprehension may be behind newly anointed Labour leader Sir Keir Starmer’s inexplicable and seemingly reflexive support for the Health Secretary’s threat on 5 April to ban all outdoor exercise if lockdown rules are not followed – a threat that probably has no basis in statute, and if carried out certainly could undermine the rule of law and citizens’ faith in it. There are sound arguments and important research questions here, about who will bear the financial costs of a prolonged lockdown and their health consequences, which have not been taken seriously enough by colleagues.
Quite apart from the material deprivation that can be anticipated as a consequence of potential economic collapse, there is the ‘loss of control over destiny’ about which Dame Margaret Whitehead and colleagues have convincingly written. Their important analysis operates on multiple scales, with the paradigmatic example of ‘pathways from traumatic social transition to poorer population health’ being the implosion of the former Soviet Union. An implosion of comparable severity, with oligarchs the primary beneficiaries, can be envisioned in the UK if both the pandemic and the retreat from lockdown are mismanaged. ‘Save lives at any cost’ is an emotionally appealing mantra, but no society anywhere, ever, has operationalised this at a population level. Destroying an economy itself has health consequences, the distribution of which will be highly unequal. An Institute for Fiscal Studies briefing shows that the lockdown will hit young workers, low-income workers and women the hardest. Impacts will also be spatially differentiated: Important research by Elena Magrini at the Centre for Cities identifies dramatic differences among cities in how many workers can adapt to work-from-home routines – or, alternatively, are vulnerable to job loss or disease exposure if they work in the essential sectors that are the unsung heroes of the pandemic. The credibility of all researchers concerned with health inequality will be defined in the coming months and years by how seriously we took these differences, and their implications for equity-oriented health, social, and economic policy – in the first instance, the design of exit strategies from the lockdown that is today in place. Those of us who did not take them seriously will no longer deserve an audience.
Imagine you’re a far-right government bent on a particular political project, whose lead minister for domestic affairs is on record as saying governments are not responsible for poverty, and you have to respond to a fast-moving contagious disease, after a decade of austerity has left the national health system overstretched even under normal circumstances and eviscerated local authorities’ ability to respond to public health crises.
You are also committed to leaving the customs union whose members buy almost half your exports and supply about 30 percent of the nation’s food, in nine months, with or without a replacement set of arrangements[1] and despite the social and economic disruption that may ensue, including disruption of food supply chains whose precariousness the epidemic is already demonstrating.
What might your sharpest-minded strategists do?
Well, one approach would start by playing down the seriousness of the epidemic. The Prime Minister might urge people to minimise social contact, whilst sometimes ignoring his own advice. As the scale and speed of the epidemic became clearer, you might go ‘evidence-based,’ relying on a particularly apocalyptic set of model predictions that ignore the possible benefits of basic public health measures such as contact tracing, clinical observation, and testing – perhaps to avoid drawing attention to austerity’s effects on the country’s ability to carry those out.
Now invoking wartime imagery, you would close schools and most businesses and public facilities countrywide. Within a few days, enabled by a hapless simpering Parliamentary opposition that did not oppose, you would enact a 348-page piece of legislation that centralises almost all power in the hands of the political executive for at least two years, and among many other extraordinary measures gives police the authority to use roadblocks and drones to prevent non-essential travel, indeed to define it, with criminal prosecution as a backstop. You would also, quite understandably, commit to massive borrowing and spending in order partially to compensate for lost jobs and business revenues, and to keep the economy from collapsing completely.
Oh, wait – the UK has such a government, and it just did all that. Lancet editor Richard Horton has written that ‘basic principles of public health and infectious disease control were ignored, for reasons that remain opaque’; the following day, former Conservative Secretary of State Jeremy Hunt made a similar point, noting – about countries that tested early and intensively – that ‘[t]he restaurants are open in South Korea. You can go shopping in Taiwan. Offices are open in Singapore’. Abundant evidence now shows that permissible movements are now determined only by police acting on their interpretation of the orders of the political executive. When the other shoe drops, in the form of post-pandemic, post-Brexit austerity that will solemnly be defended on grounds of fiscal prudence, resistance may be difficult if not dangerous. Methinks that far from blundering, the Conservative response to the pandemic has been extremely calculating and politically sophisticated. I desperately hope I’m wrong.
[1] Thanks to the US, the World Trade Organization now is nothing more than a talking shop, but that’s another story.
On the morning of 18 March, Andrew Ross Sorkin’s indispensable Dealbook blog asked ‘what a “wartime” economy looks like’, pointing to the roughly US$2.5 billion in stimulus spending that the United States, the UK, France, Germany and Spain had offered as of yesterday; warning that it might not be enough; and calling the ‘spending plans unlike anything seen during peacetime’.
Actually he’s not quite correct on that last point. The Bank of England pointed out in 2009 that in response to the financial crisis, the US and UK governments quickly mobilised an estimated US$14 trillion in cash and credit guarantees to rescue financial institutions, ‘equivalent to about 50% of annual GDP in those economies, although that does not equate to losses as in some cases these obligations were offset by holdings of assets’. It is becoming clearer by the day that a commitment of that magnitude, if not larger, will be needed to avoid a depression. And the blog points out that during the Second World War, the UK and the US ran budget deficits equivalent to more than a fifth of their respective GDPs. By 20 March, The Economist was citing a figure of US$7.4 trillion (about 23 percent of GDP) as the combined commitment from the US, the UK, Germany, France and Italy; warning that conventional fiscal policy is likely to have limited impact; and observing that ‘new financial tools need to be deployed, and fast’. An optimistic view is that Green New Deals may achieve a breadth of political support unimaginable two weeks ago.
On the other hand, Toronto’s Globe and Mail offered an important commentary pointing out that many people already living paycheque to paycheque and now facing the probability of job losses cannot afford to stockpile a fortnight’s worth of food and will probably have trouble keeping a roof over their heads – an obvious point that seems to have escaped most of the mainstream media. Both the New York Times, whose epidemic coverage is now out from behind its paywall, and the Guardian offered ominous frontline accounts calling into question the National Health Service’s ability to cope with increased caseloads after a decade of austerity-induced fragility. Similar accounts are now emerging from (among other places) the United States and Italy. And outspoken Lancet editor Richard Horton excoriated the British response as ‘a collective failure among politicians and perhaps even government experts to recognise the signals’ emanating from China and India. He concluded that ‘when we have suppressed this epidemic, when life returns to some semblance of normality, difficult questions will have to be asked and answered’.
We must now confront the possibility that, if economic policy is mismanaged and some health services collapse, that return might take, not a few years, but a generation.
In these times of plague, at least as they are categorised by some, spilling more digital ink on COVID-19 smacks of either hubris or irrelevance, and many others are better qualified than I to comment on the outbreak’s epidemiological dimensions – although, interestingly enough, they don’t always agree, and media are stretching the category of ‘scientists’. In keeping with the blog’s theme, here are a few equity-related observations.
1. In some jurisdictions, the outbreak is a neoliberal epidemic – the term Clare Bambra and I coined in 2015 – for at least two reasons. The first of these is the lack of access to paid sick leave for literally millions of low-wage US workers in retail, hospitality, and grocery sectors who either have no entitlement to paid sick leave or do not think they do, as reported by The New York Times. Of course, in the real world, for workers without a strong union this ‘entitlement’ is really at the employer’s discretion, regardless of what the law says. In the UK, the fusion of executive and legislative power gives the government of the day the ability to remedy the comparable problem instantly, if it chooses to do so. Will it?
The current outbreak is also a neoliberal epidemic because of reliance on a profit-motivated pharmaceutical industry for vaccine development. A recent journal article points out that this model for vaccine development has systematically hindered the development of vaccines for so-called neglected diseases; it may now be doing so with regard to COVID-19. In a long and important piece in The Guardian on 27 March, US researcher Peter Hotez described ‘a broken ecosystem for making vaccines’, and claimed that he might have had a COVID-19 vaccine to offer today if his team had been able to find funding for a clinical trial based on their previous (2011-2016) research on SARS. If we take seriously the broadly shared view in political theory that the most basic prerequisite for political legitimacy is a government’s ability to protect its subjects against basic threats to life and security, then the development of scientific capacity for developing diagnostics and vaccines from basic research through to production and free, not-for-profit distribution should be regarded as a national security imperative for countries able to support such initiatives, and as a development assistance priority. Will this lesson be learnt from COVID-19?
2. Focussing on the UK context, we are now seeing the consequences of a decade of austerity during which the NHS was starved for resources and the budgets of the local authorities that since 2012 have had statutory responsibility for public health have been gutted. It remains to be seen whether the NHS will be able to cope, and how high the casualty count will be both among those infected with COVID-19 and those whose care needs are displaced by COVID-19 patients in intensive care units. Rest assured, there will be casualties. In the United States, journalist Laurie Garrett has been warning for decades about the dangers of neglecting domestic public health infrastructure. In January of this year, she broke the important story that President Trump had disbanded the country’s pandemic response capability. Some mainstream media, although by no means all, have since picked up the story. Clearly, this was regarded as less important than covering promises of building big, beautiful walls to keep out threats originating in deranged racist imaginaries. Our media in the UK, and what has passed for a political opposition over the past decade, have not done a whole lot better.
3. At this writing, one UK proposal is to respond to the outbreak by isolating people over 70 in their homes for up to 16 weeks, ‘for their own protection’, which among other shortcomings defies every principle of natural justice. At this writing, it is unclear how draconian the restrictions would be, but if they are implemented, then one wonders how many deaths of despair will result not from COVID-19 infection, but from that isolation in the context of a care infrastructure that is completely unable to provide necessary support – again, after a decade of austerity.
Over the longer term, the economic impacts of the pandemic may prove to magnify health inequalities in ways that are as yet impossible to predict. For example, what happens if lengthy school closures result in job losses for parents choosing between work and leaving their children home alone? What happens to literally millions of workers in (initially) the transport, hospitality and retail sectors as their jobs disappear? What happens if, or more probably when, equity market declines mean that defined-contribution pension plans across the high-income world collapse in value and defined-benefit plans can no longer meet their obligations and face insolvency?
It is possible to envision creative and progressive (as the term is used in public finance) policy responses to all these questions, and other related ones. An International Monetary Fund researcher has called for ‘substantial targeted fiscal, monetary, and financial market measures to help affected households and businesses’ (author’s emphasis). Whether such policies will prove to be politically viable domestically and internationally given the sums involved – realistically, into trillions of US dollars – and the desirability of strongly progressive finance mechanisms is quite another question. Within their own borders, both the United States and the United Kingdom have in recent years systematically and intentionally magnified inequality and redistributed resources and opportunity upward within their social structures. Time will tell.
This post was selectively updated on 29 March; many aspects have now been overtaken by events.
I am
re-reading, not for the first time, some of the work of legal scholar Catharine
MacKinnon. (I used to refer
to her as a feminist legal scholar; I don’t do this any more, since the
adjective can be read as a qualifier, or a denigration. Scholarship is scholarship, full stop.) Her work has been an inspiration to me for a
long time, since she combines impeccable, meticulously documented philosophical
argumentation and legal reasoning with incandescent critique of injustice,
gender inequality and misogyny.
But
MacKinnon is much more than a hyper-accomplished academic. Among a host of other achievements, she was
co-counsel in the first US Supreme Court case that recognised workplace sexual
harassment as a form of discrimination; contributed to the development of
Canadian equality law under the country’s Charter
of Rights and Freedoms; was co-counsel in the suit that won a landmark US
damage award against Serbian warlord Radovan Karadzic, establishing rape as an
act of genocide in the context of ‘ethnic cleansing’; and subsequently served
as the first gender adviser to the International Criminal Court. MacKinnon’s advocacy played an important role
in generating what is now widespread recognition of rape as a weapon and
crime of war. She has written
extensively about these experiences, and much else, in a style I think of as
evidence-informed polemic. [1]
The literature on health inequity includes at least a few examples of this style. For example, in 2013 David Stuckler and Sanjay Basu argued (in The Body Economic) that: ‘The price of austerity is calculated in human lives. And these lost lives won’t return when the stock market bounces back’. Immodestly, in 2015 Clare Bambra and I put forward (in How Politics Makes Us Sick) the idea of neoliberal epidemics, specifying neoliberalism as a fundamental cause of health inequalities. And in 2017, Lancet editor Richard Horton memorably described austerity as ‘a political choice that deepens the already open and bloody wounds of the poor and precarious’. Outside the academic bubble of citation counts, these interventions (we) have had approximately zero impact in the real world. This post is an effort to start a conversation about how to change that.
One obvious
observation is that MacKinnon’s impact results from a combination of advocacy
and creative litigation using existing bodies of statute and doctrine. One of the researchers interviewed by
Katherine Smith characterised health inequalities as ‘the most
fundamental abuse of human rights in the developed world. [I]f you imagine
locking up a substantial proportion of your population for the last five or ten
years of their life without any justification at all, well actually this is
worse than that, it’s like executing them arbitrarily’. Stated thus, the point seems obvious, but it’s
hard to see avenues for turning it into a basis for litigation. Maybe concerned academics have simply not
connected with the right litigators, but issues of causation might present
formidable barriers to success, given courts’ (and many epidemiologists’)
tendency to set standards of proof that are often
inappropriately high.
At least in the UK, the deliberate corruption of universities
by organising priorities and career paths around generating research income means
fewer and fewer academics – mainly those near the end of their working lives,
without dependents or with independent wealth – can engage in evidence-informed
polemic rather than forelock-tugging before funders without fear of
reprisal. Professionals working in
public health in government are likely to be even more limited in their ability
to speak out, however sophisticated their private understandings of the origins
and politics of health inequality (and in many cases, again in the UK at least,
these are very sophisticated indeed). The tendency of too many health promoters to acquiesce in
the popular conception of poor health as somehow the fault of the
individual affected does not help.
Perhaps the most important issue is suggested by Sir Michael
Marmot’s call, after the release of the 2008 WHO Commission report, for ‘a
social movement, based on evidence, to reduce inequalities in health’. That movement has yet to materialise. Writing about women’s resistance to workplace
sexual harassment in the United States, Carrie
Baker defines social movements as ‘a mixture of informal networks and
formal organizations outside of conventional politics that make clear demands
for fundamental social, political, or economic change and utilize
unconventional or protest tactics’. Crucially,
many coalitions that formed to fight sexual harassment connected women who were not otherwise similarly situated
in socioeconomic terms. Another, much more recent manifestation of
such a coalition is the powerful anti-violence performance ‘A rapist in your path’, which
originated in last autumn’s Chilean protests against inequality and has now gone viral in much of the world.
Here’s the
rub. As I wrote a decade ago in the
Canadian context, effective social movements need not only evidence and
coalitions, but also rage, hopelessness, desperation, hope, shared passion,
shared vulnerabilities, or some combination of these. That’s where their energy comes from. If one adopts a suitably precautionary
standard of proof, as suggested by the human rights frame, there is no shortage
of evidence – certainly not of the damage done by the past decade’s systematic
upward redistribution of resources and opportunity. What possible coalitions could move the
health equity agenda forward, and how can the necessary emotional energy be mobilised? Let the conversation begin.
[1] A
selection of MacKinnon’s earlier work appears in Feminism,
Unmodified (1988); somewhat later work in Are Women
Human? (2007); and her landmark explication of feminism as political theory
in Toward
a Feminist Theory of the State (1991). A very recent open access introduction to her
perspective is available here.
Most readers will now be aware of the release on 25 February of the ten-year followup to the 2010 ‘Marmot review’ of health inequalities in England. To say that the report makes depressing reading is putting it mildly. Despite the epidemiologist’s caution expressed in Sir Michael Marmot’s foreword – ‘We were reluctant to attribute the slowdown in health improvement to years of austerity because of difficulty in establishing cause and effect – we cannot repeat years without austerity just to test a hypothesis’ – the report as a whole offers a devastating portfolio of evidence of the human damage done by a decade of austerity. Its accumulation of graphs and charts makes a compelling case for the point I try to bring home to postgraduate students at every opportunity: public finance is a public health issue. An especially bitter irony, of course, is the emerging recognition across much of the political spectrum, and of the economics profession, that the decade was not only unnecessary but even counterproductive in macroeconomic terms.
Unfortunately, that kind of evidence is not relevant to the broader post-2010 project of redistributing income, wealth, and opportunity upward within British society. (The brilliant and iconoclastic economist Branko Milanovic has pointed out that the rich have much more to gain from such upward redistribution than from stimulating growth across an entire national economy; their ready access to tax avoidance opportunities unavailable to the rest of us further distorts the incentive structure.) Neither does evidence of macroeconomic (in)effectivess bear on what might be called the micro-level attack on the poor, marginalised and precarious. The day after the release of Marmot +10, The Independent reported that the Department of Work and Pensions had shredded ‘up to 49’ internal reviews of suicides that occurred after people’s benefits had been cut off. This followed an earlier report of 69 suicides among benefit claimants in the past five years, which is almost certainly a low figure.
Just a few
items from the report deserve flagging.
Fewer than 200,000 workers in the UK were on zero hours contracts in
2010; by late 2018 the figure was close to 900,000. For the poorest tenth of English households,
eating healthily would require three-quarters of all their disposable income after housing costs. And the targeted financial destruction of
local government has led (for example) to an England-wide reduction of 42
percent in local spending on transport and a 52 percent cut in housing. As the report points out, ‘councils have used
reserves, sold assets and reduced spending on the non-statutory services they
are not legally required to deliver’.
None of
this matters to Mr. and Mrs. Range Rover, of course. An Arizonan interviewed by US journalist Ken
Silverstein captured
the underlying political economy a decade ago: ‘People who have swimming pools
don’t need state parks. If you buy your books at Borders you don’t need
libraries. If your kids are in private school, you don’t need K-12. The people
here, or at least those who vote, don’t see the need for government.’ And The
Timesrecently
reported that residents in some of London’s ultra-wealthy boroughs pay less
than £1 in council tax for every £1,000 of property value, whilst those in ten
poor local authorities in the Midlands and the North such as Hartlepool,
Middlesbrough, Gateshead and Stockton-on-Tees pay between ten and fourteen
times as much (unfortunately behind a paywall; contact me if you would like the
figures.)
It is hard to know how to respond to such
situations, beyond despair and resignation.
These responses are heightened by the fact that many of the new report’s
‘case studies,’ seemingly intended as success stories, are at best sticking
plasters, doing little to address the critical upstream drivers of inequality –
the ‘toxic combination of poor social policies and programmes, unfair economic
arrangements, and bad politics’ correctly targeted by the 2008 Commission on
Social Determinants of Health. I have to
remind myself more and more often that the last word in Albert Camus’ famous
essay on suicide is hope. One hope is
that public health researchers and practitioners might disengage themselves
from producing yet more systematic reviews of the evidence, organised around
impossibly and inappropriately high epidemiological
standards of proof, and turn attention, energy and pedagogy to more
practical questions such as what to do when government adopts homicidal social
policies and then destroys the evidence.
The news of the day sometimes throws up events that combine to
highlight the absurdity, and the perversity, of today’s policies of selective
market fundamentalism.
Tuesday, 14 January was one of those days. The
Guardian reported that councillors in the last county in England without a
Burger King, Kentucky Fried Chicken or McDonald’s restaurant (if that is really
the appropriate word) had
approved a 24-hour McDonald’s drive-through in the town of
Oakham. This happened even though 55 of
the 78 representations submitted to planning officers opposed the planning
permission.
In a spirit of rough and ready critical discourse analysis,
it is worth considering the language of the news report. Damien Gayle and Kevin Rawlinson wrote that
many people they interviewed were ‘hopeful that the new restaurant would give
the town’s young people somewhere to go
and create local jobs’ (my italics), and ‘[p]arents … said they would welcome
not having to drive to neighbouring
counties to “treat” their children to McDonald’s food’ (my italics again).
So this is what market fundamentalism hath wrought, and obeisance before the deity of (private sector) job creation is only part of the picture. Silly me; I would never have thought of McDonald’s on a list of places for young people to go. Oakham’s library is still functioning, unlike the 343 libraries across the UK that closed between 2010 and 2015, although admittedly it is only open during the day Monday to Saturday. Rutland County’s web site offers numerous links to parking information, but no mention of parks; I’m not certain what to make of that. And these are strange days indeed when parents feel compelled to drive substantial to feed their children a McDonald’s meal. The industry, of course, is not just a passive bystander. It targets children in its advertising, as McDonald’s did in Chile; this was pointed out in the web summary of a September 2011 Euromonitor report that is no longer online, but I have it on file.
‘McDonald’s arrived in Chile targeting the segment of children, but over time, the customer base has expanded from not just children to also their parents, as well as young people. This strategy has allowed this brand to claim an important part of the category, and it has established itself amongst consumers of fast food ’ (Euromonitor, 2011; photo from Santiago city centre: T. Schrecker)
On, then, to the second news item of the day. Short-haul airline Flybe, which serves
56 locations in the UK and continental Europe, received a bailout
from its major shareholders that may be accompanied by sweeteners
from the magic public money tree including deferred tax payments and
a reduction in air passenger duty on domestic flights. Entirely understandable expressions of
outrage, not least from its commercial competitors, seem likely to have no
effect, yet as Nils
Pratley pointed out in The
Guardian: ‘Increased trading losses? Higher fuel costs after sterling’s
decline last summer? Brexit uncertainty?
None of those risks were unimaginable 12
months ago’. This is a case of bad management, or more accurately
bad accounting, pure and simple. Management
is surely what was lacking.
It’s as if no one had heard of climate change, or the
aviation industry’s contribution to greenhouse gas emissions.
Many forms of infrastructure are essential for modern life, and in the UK many have been dismembered by a decade of austerity. In a carbon-conscious age when, as economists never cease to remind us, resources are limited, a failing regional airline is not one of those essentials. The idea of letting markets work never seems to play very well in the commercial aviation industry, or with its political protectors.
Now, please don’t take what I am about to write the wrong
way. All of us concerned with health
inequalities recognise that governments must get in the way of markets, in all
kinds of ways and for all kinds of reasons.
But here are two modest proposals, with apologies to Jonathan Swift, for
how a creative, environment- and health-friendly government might use markets
to move towards a healthier, less inequitable and greener world.
First: let airlines, like your local drycleaner, price their
services at a level that will ensure an adequate return on investment, whatever
that may be, or go bust. By all means
subsidise transport, but concentrate on options that generate the fewest
negative health impacts: low-carbon rail
and bus services, active transport, and reducing the need for travel. Conversely, massively dis-incentivise
polluting and carbon-intensive transport.
The British Heart Foundation have just launched an
important campaign on air pollution, as
has The Times; more power to them
both, even though The Times’s
proposals are modest, perhaps in deference to its Range Rover readership.
Second: if planning
permission for fast food franchises must be allowed, why can’t central
government legislate a quota of such permissions for the entire country, or for
each region (say, in the English case, each NHS
footprint area); auction opportunities to apply for them to the
highest bidders, with periodic renewal required; and gradually shrink the quota
at each successive auction? The tidy bit
of revenue generated could be ring-fenced to reopen libraries and activity
centres, restore parks, use traffic calming to improve the activity-friendliness
of neighbourhoods, and perhaps subsidise the cost of healthy food.
With the
election over and the United Kingdom’s exit from the European Union on some
terms or other now a certainty, it is useful to reflect on the trade
negotiations that will follow. I offer
these initial observations.
First, there has been much talk of the option of reverting to World Trade Organization (WTO) rules in trade relations if ‘deals’ to replace the agreements to which the UK was party by virtue of its EU membership cannot be negotiated by the end of 2020. However, thanks to the United States’ refusal to agree to appointing new members of the WTO Appellate Body, effectively there will be no WTO rules going forward, until and unless a future US government changes this position in 2021 or thereafter. Once out of the EU, the UK is effectively unprotected in a trade policy jungle, not having been able to negotiate independently of the EU, so pressure quickly to negotiate new agreements will be intense. Domestic proponents of a deregulated, ultra-liberal future, including (for example) further privatisation in the NHS and opening the country’s arms even wider to dodgy flight capital, will make use of this opportunity. The government’s announced intent to legislate an exit from the EU at the end of 2020, whether or not an agreement has been reached, is a first step in this process.
Second, in
this process the UK will be at a substantial disadvantage as it negotiates with
entities like the United States (an economy more than six times larger, based on GDP at purchasing power
parity) and the comparably large European Union.
It will have to offer more, in terms of market access and other
considerations, to get less. And when
anyone in an official capacity says that a particular service or health
protection measure, such as the NHS or food safety standards, ‘will not be on
the table’, we have to ask what else will be on the table instead. That is the reality of asymmetrical trade
negotiations, as countries throughout the Global South have found out.
Third, the House of Commons will be largely irrelevant. A former Canadian cabinet minister pointed out decades ago that: ‘Under our parliamentary system, a Prime Minister or a Premier with a majority has immense power …. [In] 1688 we traded the divine right of kings for the divine right of a Premier or a Prime Minister with a majority at his or her back for a period of five years’. The new Conservative government has a large enough majority that even with a unanimous opposition, close to 40 defections would be necessary in order to defeat whatever legislation the government proposed, and that is all but unthinkable. Advocates for health equity concerned with the implications of post-Brexit trade policy will have to look elsewhere for points of influence. There may not be many.
Thus, fourth, a final irony. The campaign to leave the EU was waged using the mantra of taking back control. During the process of leaving and after its completion, influences and actors outside the UK’s border will probably be more important in terms of shaping the direction of the economy, society and everyday life than they were during the country’s EU membership.