
Dr Toby Lowe from the Centre for Knowledge, Innovation, Technology and Enterprise (Newcastle University Business School) presents his Idea for an Incoming Government: make public services more effective. He urges us to move away from a ‘Payment by Results’ approach, and suggests alternatives that would cope better with the messiness of the problems we face in our society.
What is the problem?
Governments have attempted to make public services more accountable for producing desirable social outcomes. From reducing reoffending to helping the long-term unemployed to find work increasing numbers of programmes are commissioned using a ‘Payment by Results’ approach (PbR).
The rationale behind seems compelling – we should only pay for work undertaken that is effective in solving the problems that society has identified. Unfortunately, the evidence suggests that PbR creates a paradox – programmes commissioned on this basis produce worse results, particularly for those with the most complex needs.
There are two reasons why this is the case:
Firstly, real life is complex and messy. But PbR programmes need life to be simple and measurable. They require that desired ‘outcomes’ can be easily measured – because payments are triggered by these measures. Unfortunately, the complex social issues which social interventions most often deal with are frequently those that are most difficult to measure. Take, for example, tackling obesity. Body Mass Index (BMI) is the measure that is most frequently used to measure obesity. It is used a measure of obesity because it is easy to measure: it is a simple measure of weight in proportion to height. Anyone with a BMI of more than 25 is overweight. Anyone with a BMI of more than 30 is obese.
Unfortunately, real obesity is much more complicated than that. BMI doesn’t effectively measure obesity for children, individuals with different body shapes, with different exercise regimes, and with certain medical conditions. According to BMI measures, this woman, Anita Albrecht, who is a personal trainer, is very overweight, and is only one BMI point short of being clinically obese.

So what happens if you use what is measurable as mechanisms to pay by results? You end up wasting time and money targeting obesity programmes on people like Anita – because that’s what simple targets, which are abstracted from the intrinsic messiness and complexity of life make people do.
The second reason that PbR makes it more difficult to create good outcomes is that they work on very simple cause and effect logic: if you are going to pay a person or organisation for producing a result, then you need to know that it was that person or that organisation which did it. How else do you know who to pay?
Unfortunately, the messiness of real life gets in the way once more. Real outcomes are emergent properties of complex systems. Look at the complex system which lies behind obesity as an issue:
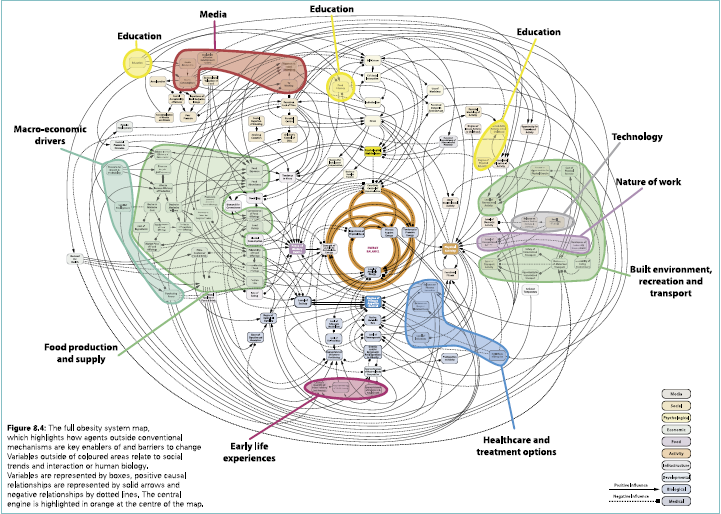
This is the reality of what causes obesity. If you pay an organisation to undertake obesity activity, they can only influence a small part of this system. Whether people actually end up obese or not is the result of the interaction of a hundred other factors.
If you pay people or organisations on the basis of whether they achieve particular results, you are asking them to be accountable for things they don’t control. As a result, they learn to manage what they can control – which is the production of data. This is the evidence about what people do: They reclassify what counts as success (for example, counting trolleys as beds in hospitals in order to meet waiting time targets). They only work on clients who they know will provide the desired results, and they ignore the more difficult clients. They ‘teach to the test’ – only doing things which relate to what is measured, ignoring people’s needs that don’t fit into the simple measurement framework. And if all else fails, they simply make up data.
They do this because Payment by Results is nothing of the sort. Payment by Results should really be called ‘Payment for Data Production’. It changes the purpose of people’s job from helping those in need to producing the data which gets them paid.
All this is an enormous waste of resources. We end up paying huge fees to organisations who can play the data production game well, rather than those who are good at helping people. We waste resources paying organisations not to help those most in need.
The solution
The evidence is clear. If you want to achieve good outcomes, don’t pay by results. Evidence shows that these alternative approaches are successful:
1) Use systems thinking and invest in relationships. Design systems around people’s needs. Invest in organisations that build relationships with clients, and so who understand their needs authentically. Commission locally, so that the organisations have a connection with the people they serve.
2) Promote horizontal accountability. Make practitioners accountable to one another for the quality of their work. Create mechanisms for peer-based critical reflection, such as Learning Communities.
3) Create positive error cultures. Create cultures in which people talk honestly about uncertainty and mistakes – because this is how people learn and improve.


{kind=link}